Holubar Stefan D, Hedrick Traci, Gupta Ruchir, Kellum John, Hamilton Mark, Gan Tong J, Mythen Monty G, Shaw Andrew D, Miller Timothy E
Department of Surgery, Dartmouth-Hitchcock Medical Center, Lebanon, NH USA.
Department of Surgery, University of Virginia Health System, Charlottesville, VA USA.
Perioper Med (Lond). 2017 Mar 3;6:4. doi: 10.1186/s13741-017-0059-2. eCollection 2017.
Colorectal surgery (CRS) patients are an at-risk population who are particularly vulnerable to postoperative infectious complications. Infectious complications range from minor infections including simple cystitis and superficial wound infections to life-threatening situations such as lobar pneumonia or anastomotic leak with fecal peritonitis. Within an enhanced recovery pathway (ERP), there are multiple approaches that can be used to reduce the risk of postoperative infections.
With input from a multidisciplinary, international group of experts and through a focused (non-systematic) review of the literature, and use of a modified Delphi method, we achieved consensus surrounding the topic of prevention of postoperative infection in the perioperative period for CRS patients.
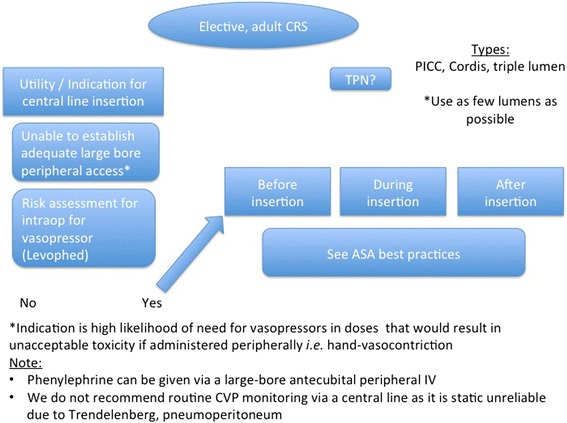
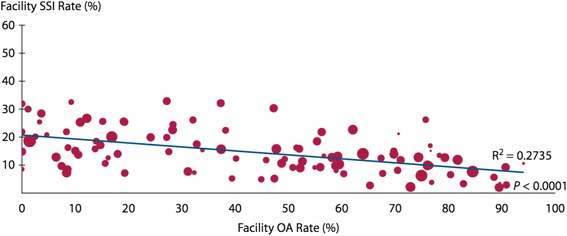
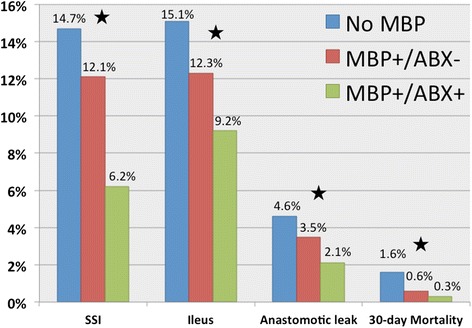
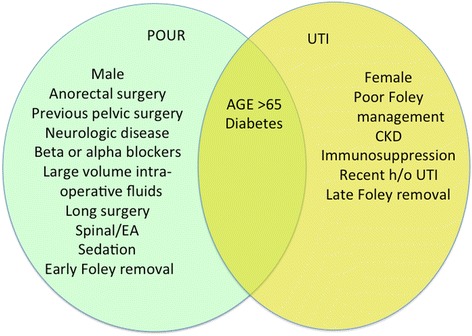
As a part of the first Perioperative Quality Initiative (POQI-1) workgroup meeting, we sought to develop a consensus statement describing a comprehensive, yet practical, approach for reducing postoperative infections, specifically for CRS within an ERP. Surgical site infection (SSI) is the most common postoperative infection. To reduce SSI, we recommend routine use of a combined isosmotic mechanical bowel preparation with oral antibiotics before elective CRS and that infection prevention strategies (also called bundles) be routinely implemented as part of colorectal ERPs. We recommend against routine use of abdominal drains. We also give consensus guidelines for reducing pneumonia, urinary tract infection, and central line-associated bloodstream infection (CLABSI).
结直肠手术(CRS)患者属于高危人群,特别容易发生术后感染性并发症。感染性并发症范围从轻微感染,包括单纯膀胱炎和浅表伤口感染,到危及生命的情况,如大叶性肺炎或伴有粪性腹膜炎的吻合口漏。在强化康复路径(ERP)中,有多种方法可用于降低术后感染风险。
在一个多学科的国际专家小组的参与下,通过对文献进行重点(非系统性)回顾,并采用改良的德尔菲法,我们就CRS患者围手术期预防术后感染这一主题达成了共识。
作为首个围手术期质量倡议(POQI-1)工作组会议的一部分,我们试图制定一份共识声明,描述一种全面而实用的方法来减少术后感染,特别是针对ERP中的CRS。手术部位感染(SSI)是最常见的术后感染。为减少SSI,我们建议在择期CRS前常规使用等渗机械性肠道准备联合口服抗生素,并将感染预防策略(也称为集束化措施)作为结直肠ERP的一部分常规实施。我们不建议常规使用腹腔引流管。我们还给出了减少肺炎、尿路感染和中心静脉导管相关血流感染(CLABSI)的共识指南。