Chau Elaine M T, Manns Braden J, Garg Amit X, Sood Manish M, Kim S Joseph, Naimark David, Nesrallah Gihad E, Soroka Steven D, Beaulieu Monica, Dixon Stephanie, Alam Ahsan, Tangri Navdeep
Chronic Disease Innovation Centre, Seven Oaks General Hospital, Winnipeg, Manitoba, Canada; Department of Internal Medicine, University of Manitoba, Winnipeg, Canada.
Department of Medicine, University of Calgary, Alberta, Canada.
Can J Kidney Health Dis. 2016 Sep 14;3:2054358116665257. doi: 10.1177/2054358116665257. eCollection 2016.
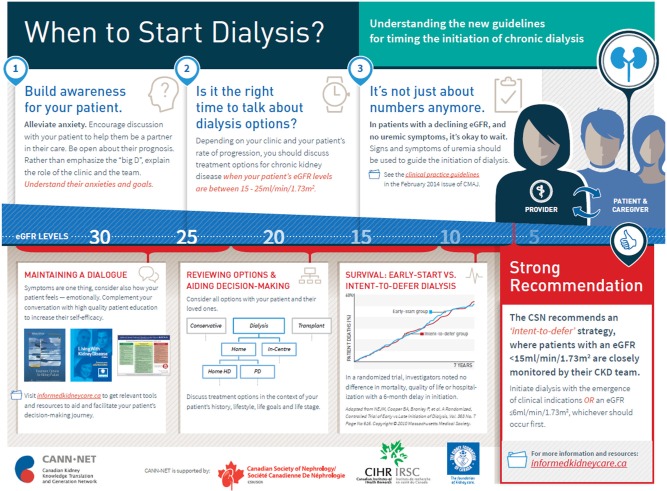
Early initiation of chronic dialysis (starting dialysis with higher vs lower kidney function) has risen rapidly in the past 2 decades in Canada and internationally, despite absence of established health benefits and higher costs. In 2014, a Canadian guideline on the timing of dialysis initiation, recommending an intent-to-defer approach, was published.
The objective of this study is to evaluate the efficacy and safety of a knowledge translation intervention to promote the intent-to-defer approach in clinical practice.
This study is a multicenter, 2-arm parallel, cluster randomized trial.
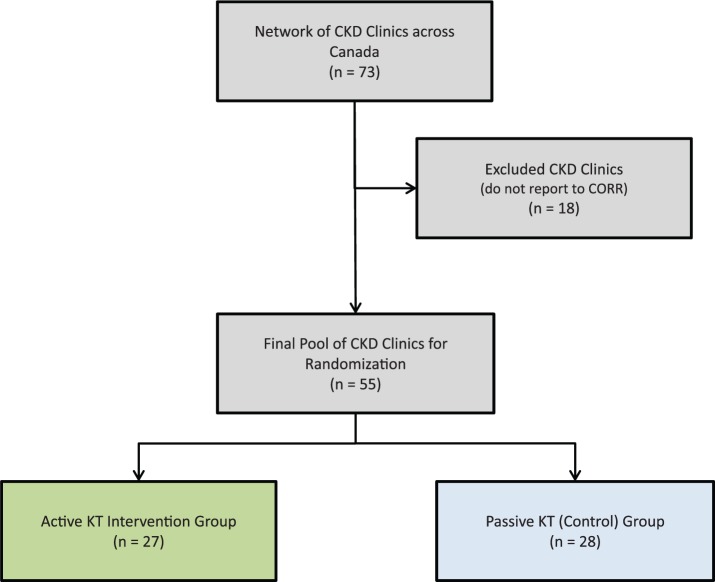
The study involves 55 advanced chronic kidney disease clinics across Canada.
Patients older than 18 years who are managed by nephrologists for more than 3 months, and initiate dialysis in the follow-up period are included in the study.
Outcomes will be measured at the patient-level and enumerated within a cluster. Data on characteristics of each dialysis start will be determined by linkages with the Canadian Organ Replacement Register. Primary outcomes include the proportion of patients who start dialysis early with an estimated glomerular filtration rate greater than 10.5 mL/min/1.73 m and start dialysis in hospital as inpatients or in an emergency room setting. Secondary outcomes include the rate of change in early dialysis starts; rates of hospitalizations, deaths, and cost of predialysis care (wherever available); quarterly proportion of new starts; and acceptability of the knowledge translation materials.
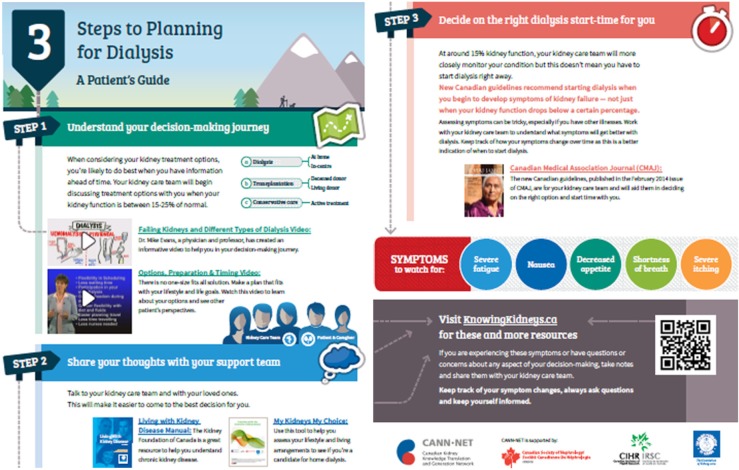
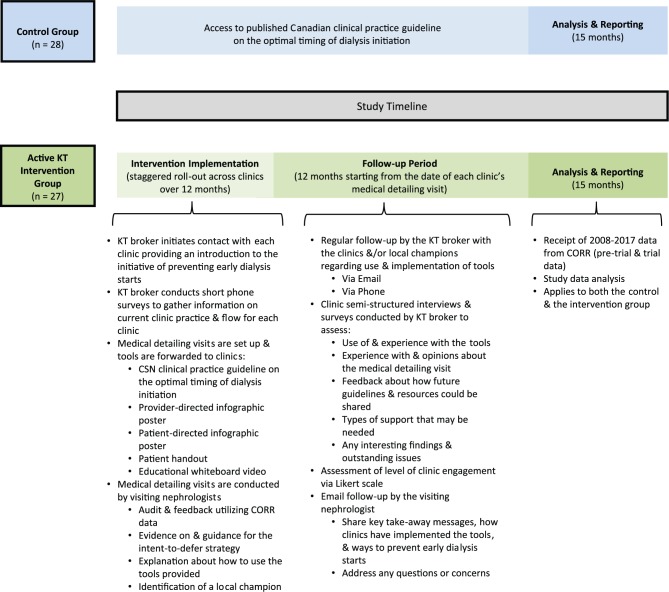
We randomized 55 multidisciplinary chronic disease clinics (clusters) in Canada to receive either an active knowledge translation intervention or no intervention for the uptake of the guideline on the timing of dialysis initiation. The active knowledge translation intervention consists of audit and feedback as well as patient- and provider-directed educational tools delivered at a comprehensive in-person medical detailing visit. Control clinics are only exposed to guideline release without active dissemination. We hypothesize that the clinics randomized to the intervention group will have a lower proportion of early dialysis starts.
Limitations include passive dissemination of the guideline through publication, and lead-time and survivor bias, which favors delayed dialysis initiation.
If successful, this active knowledge translation intervention will reduce early dialysis starts, lead to health and economic benefits, and provide a successful framework for evaluating and disseminating future guidelines.
ClinicalTrials.gov, NCT02183987.
在过去20年里,加拿大及国际上慢性透析的早期启动(在肾功能较高或较低时开始透析)迅速增加,尽管尚无明确的健康益处且成本更高。2014年,加拿大发布了一项关于透析启动时机的指南,推荐采用延迟透析的方法。
本研究的目的是评估一项知识转化干预措施在临床实践中推广延迟透析方法的有效性和安全性。
本研究是一项多中心、双臂平行、整群随机试验。
该研究涉及加拿大各地的55家晚期慢性肾脏病诊所。
由肾病科医生管理超过3个月且在随访期内开始透析的18岁以上患者纳入本研究。
结局将在患者层面进行测量,并在一个群组内进行统计。每次透析开始的特征数据将通过与加拿大器官替代登记处的关联来确定。主要结局包括估计肾小球滤过率大于10.5 mL/min/1.73 m²时早期开始透析且作为住院患者或在急诊室环境中开始透析的患者比例。次要结局包括早期透析开始的变化率;住院率、死亡率和透析前护理费用(如有);新开始透析的季度比例;以及知识转化材料的可接受性。
我们将加拿大的55家多学科慢性病诊所(群组)随机分为两组,一组接受积极的知识转化干预,另一组不接受关于透析启动时机指南的推广干预。积极的知识转化干预包括审核与反馈以及在全面的面对面医学详情介绍访问中提供的针对患者和提供者的教育工具。对照诊所仅接触到指南发布,而没有积极传播。我们假设随机分配到干预组的诊所早期透析开始的比例会更低。
局限性包括通过出版物被动传播指南,以及领先时间和幸存者偏倚,这有利于延迟透析启动。
如果成功,这种积极的知识转化干预将减少早期透析开始,带来健康和经济效益,并为评估和传播未来指南提供一个成功的框架。
ClinicalTrials.gov,NCT02183987。