Department of Pediatrics, Children's National Medical Center, Washington, DC.
Department of Pediatrics, University of Utah School of Medicine, Salt Lake City, Utah.
J Thorac Cardiovasc Surg. 2017 Aug;154(2):620-628.e6. doi: 10.1016/j.jtcvs.2017.01.050. Epub 2017 Feb 10.
Outcome prediction for pediatric heart surgery has focused on mortality but mortality has been significantly reduced over the past 2 decades. Clinical care practices now emphasize reducing morbidity. Physiology-based profiles assessed by the Pediatric Risk of Mortality (PRISM) score are associated with new significant functional morbidity detected at hospital discharge. Our aims were to assess the relationship between new functional morbidity and surgical risk categories (Risk Adjustment for Congenital Heart Surgery [RACHS] and Society for Thoracic Surgery Congenital Heart Surgery Database Mortality Risk [STAT]), measure the performance of 3-level (intact survival, survival with new functional morbidity, or death) and 2-level (survival or death) PRISM prediction algorithms, and assess whether including RACHS or STAT complexity categories improves the PRISM predictive performance.
Patients (newborn to age 18 years) were randomly selected from 7 sites (December 2011-April 2013). Morbidity (using the Functional Status Scale) and mortality were assessed at hospital discharge. The most recently published PRISM algorithms were tested for goodness of fit, and discrimination with and without the RACHS and STAT complexity categories.
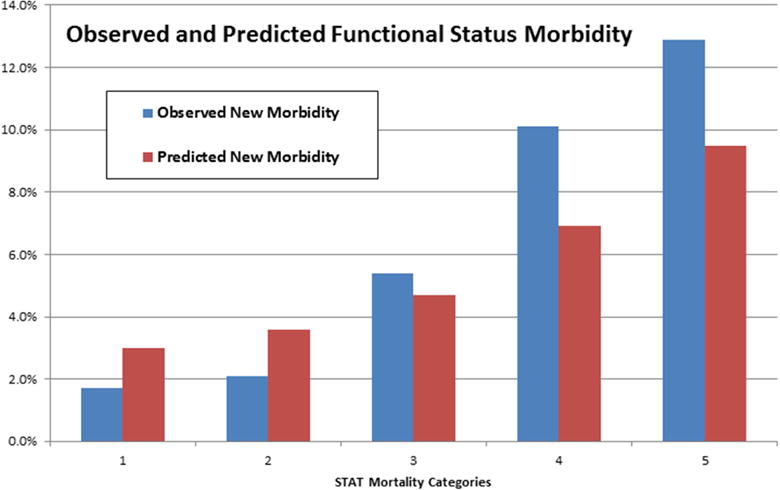
The mortality rate in the 1550 patients was 3.2%. Significant new functional morbidity rate occurred in 4.8%, increasing from 1.8% to 13.9%, 1.7%, and 12.9% from the lowest to the highest RACHS and STAT categories, respectively. The 3-level and 2-level PRISM models had satisfactory goodness of fit and substantial discriminative ability. Inclusion of RACHS and STAT complexity categories did not improve model performance.
Both mortality and new, functional morbidity are important outcomes associated with surgical complexity and can be predicted using PRISM algorithms. Adding surgical complexity to the physiologic profiles does not improve predictor performance.
儿科心脏手术的预后预测一直集中在死亡率上,但在过去的 20 年中,死亡率已经显著降低。临床护理实践现在强调降低发病率。儿科死亡率风险评分(PRISM)评估的基于生理学的评分与在出院时检测到的新的显著功能发病率相关。我们的目的是评估新的功能发病率与手术风险类别(先天性心脏手术风险调整 [RACHS] 和胸外科先天性心脏手术数据库死亡率风险 [STAT])之间的关系,衡量 3 级(完整存活率、存活伴有新的功能发病率或死亡)和 2 级(存活或死亡)PRISM 预测算法的性能,并评估是否包含 RACHS 或 STAT 复杂类别是否能提高 PRISM 预测性能。
从 7 个地点(2011 年 12 月至 2013 年 4 月)随机选择患者(新生儿至 18 岁)。在出院时评估发病率(使用功能状态量表)和死亡率。测试了最新发表的 PRISM 算法的拟合优度和有无 RACHS 和 STAT 复杂类别时的区分能力。
在 1550 名患者中,死亡率为 3.2%。新的功能发病率发生率为 4.8%,从最低到最高的 RACHS 和 STAT 类别,分别增加到 1.8%、13.9%、1.7%和 12.9%。3 级和 2 级 PRISM 模型具有良好的拟合优度和较大的区分能力。包含 RACHS 和 STAT 复杂类别并不能提高模型性能。
死亡率和新的功能发病率都是与手术复杂性相关的重要预后,可使用 PRISM 算法进行预测。将手术复杂性添加到生理特征中并不能提高预测器的性能。