Schoemaker Rik, Wade Janet R, Stockis Armel
SGS Exprimo, Mechelen, Belgium.
Occams, Malandolaan 10, 1187, HE, Amstelveen, The Netherlands.
Eur J Clin Pharmacol. 2017 Jun;73(6):727-733. doi: 10.1007/s00228-017-2230-6. Epub 2017 Mar 9.
The aims of the study were to develop a population pharmacokinetic model of orally administered brivaracetam in paediatric patients and to provide dosing suggestions.
Analysis included 600 brivaracetam plasma concentrations from a phase 2a study (NCT00422422; N01263) in 96 paediatric patients with epilepsy aged 1 month to 16 years, taking one to three concomitant antiepileptic drugs (AEDs). Pharmacokinetic analysis was performed using non-linear mixed effects modelling, and a stepwise covariate search was used to determine factors influencing brivaracetam clearance. Simulations were performed to investigate dosing regimens.
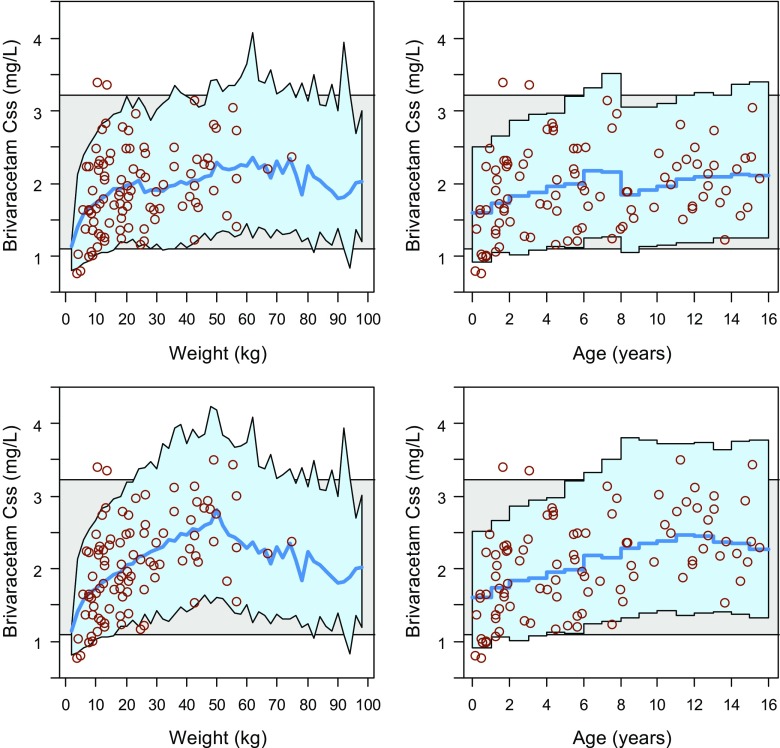
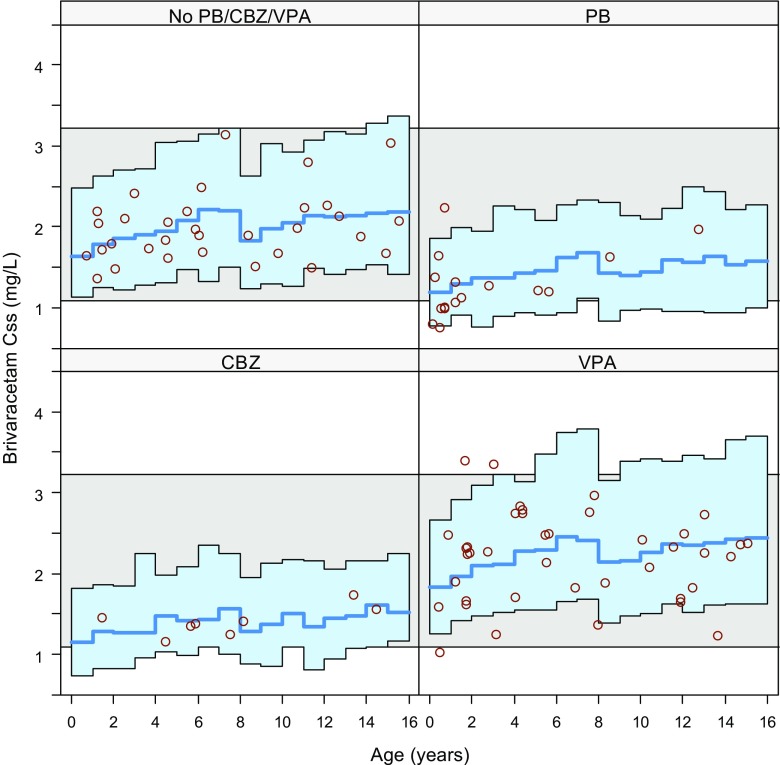
The final model consisted of first-order absorption, single compartment distribution and first-order elimination components with allometric scaling of clearance and volume using lean body weight and fixed allometric exponents. Co-administration with phenobarbital or carbamazepine was associated with a 29% (95%CI 17%/39%) and 32% (22%/42%) decrease in exposure, respectively. Co-administration with valproate was associated with an 11% (1%/23%) increase in exposure. Simulations demonstrated that the majority of children were predicted to have an exposure similar to that in adults, using an age-independent dosing regimen of 2.0 mg/kg bid with a maximum of 100 mg bid for body weight >50 kg.
A paediatric dose adaptation of 2.0 mg/kg twice daily with a maximum of 100 mg twice daily for body weight >50 kg is predicted to ensure steady-state plasma concentrations in the same range as in adult patients receiving 100 mg twice daily (highest recommended dose). Data suggest no need to change brivaracetam dosing when used concomitantly with carbamazepine, phenobarbital or valproate.
本研究旨在建立小儿患者口服布瓦西坦的群体药代动力学模型,并提供给药建议。
分析纳入了一项2a期研究(NCT00422422;N01263)中的600份布瓦西坦血浆浓度数据,该研究涉及96例年龄在1个月至16岁的癫痫小儿患者,这些患者同时服用1至3种抗癫痫药物(AEDs)。采用非线性混合效应模型进行药代动力学分析,并通过逐步协变量搜索来确定影响布瓦西坦清除率的因素。进行模拟以研究给药方案。
最终模型由一级吸收、单室分布和一级消除组分构成,清除率和容积采用基于瘦体重的异速生长标度及固定的异速生长指数。与苯巴比妥或卡马西平合用分别使暴露量降低29%(95%CI 17%/39%)和32%(22%/42%)。与丙戊酸合用使暴露量增加11%(1%/23%)。模拟表明,对于体重>50 kg的儿童,采用2.0 mg/kg bid的年龄无关给药方案,最大剂量为100 mg bid,预计大多数儿童的暴露量与成人相似。
预计对于体重>50 kg的儿童,采用2.0 mg/kg每日两次、最大剂量为100 mg每日两次的儿科剂量调整方案可确保稳态血浆浓度与接受每日两次100 mg(最高推荐剂量)的成人患者处于同一范围。数据表明,与卡马西平、苯巴比妥或丙戊酸合用时无需调整布瓦西坦剂量。