Feldstein David A, Hess Rachel, McGinn Thomas, Mishuris Rebecca G, McCullagh Lauren, Smith Paul D, Flynn Michael, Palmisano Joseph, Doros Gheorghe, Mann Devin
Division of General Internal Medicine, University of Wisconsin School of Medicine and Public Health, 2828 Marshall Court, Suite 100, Madison, WI, 53705, USA.
Division of Health System Innovation and Research, University of Utah School of Medicine, Williams Building, 295 Chipeta Way, Salt Lake City, UT, 84108, USA.
Implement Sci. 2017 Mar 14;12(1):37. doi: 10.1186/s13012-017-0567-y.
Clinical prediction rules (CPRs) represent a method of determining individual patient risk to help providers make more accurate decisions at the point of care. Well-validated CPRs are underutilized but may decrease antibiotic overuse for acute respiratory infections. The integrated clinical prediction rules (iCPR) study builds on a previous single clinic study to integrate two CPRs into the electronic health record and assess their impact on practice. This article discusses study design and implementation of a multicenter cluster randomized control trial of the iCPR clinical decision support system, including the tool adaptation, usability testing, staff training, and implementation study to disseminate iCPR at multiple clinical sites across two health care systems.
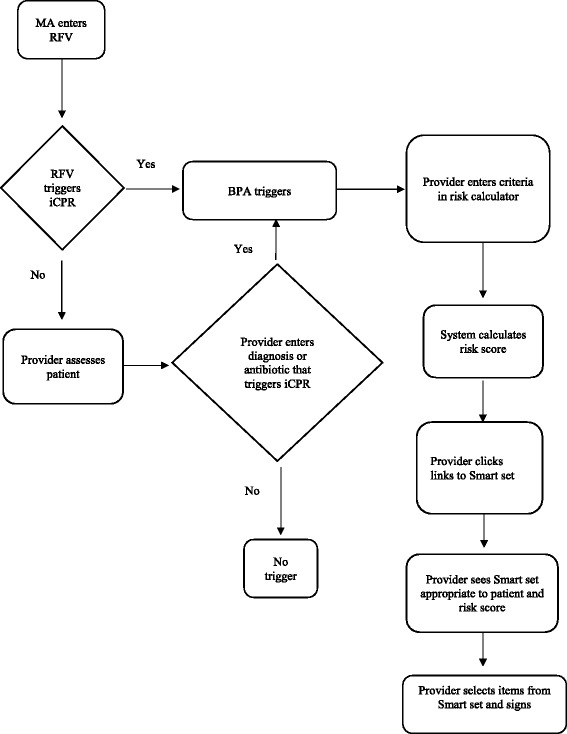
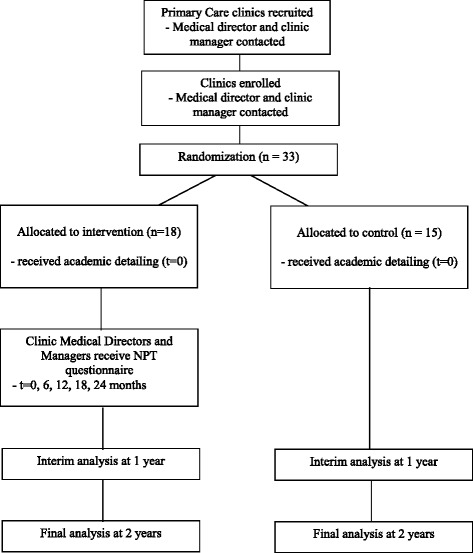
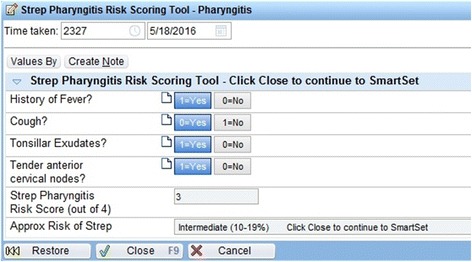
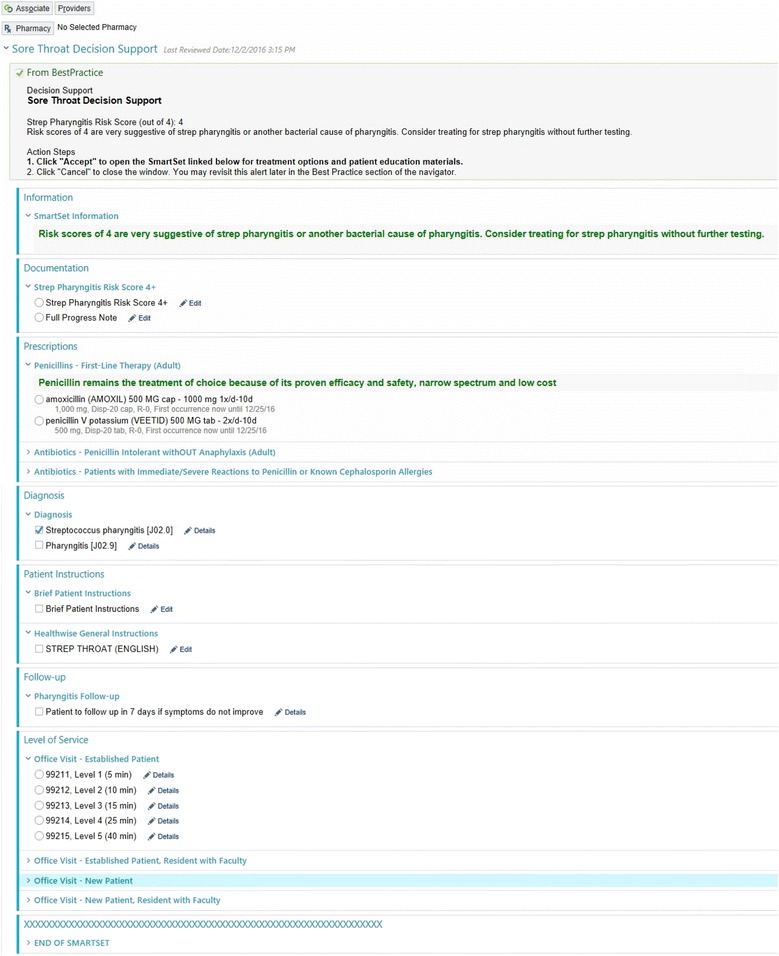
The iCPR tool is based on two well-validated CPRs, one for strep pharyngitis and one for pneumonia. The iCPR tool uses the reason for visit to trigger a risk calculator. Provider completion of the risk calculator provides a risk score, which is linked to an order set. Order sets guide evidence-based care and include progress note documentation, tests, prescription medications, and patient instructions. The iCPR tool was refined based on interviews with providers, medical assistants, and clinic managers, and two rounds of usability testing. "Near live" usability testing with simulated patients was used to ensure that iCPR fit into providers' clinical workflows. Thirty-three Family Medicine and General Internal Medicine primary care clinics were recruited at two institutions. Clinics were randomized to academic detailing about strep pharyngitis and pneumonia diagnosis and treatment (control) or academic detailing plus use of the iCPR tool (intervention). The primary outcome is the difference in antibiotic prescribing rates between the intervention and control groups with secondary outcomes of difference in rapid strep and chest x-ray ordering. Use of the components of the iCPR will also be assessed.
The iCPR study uses a strong user-centered design and builds on the previous initial study, to assess whether CPRs integrated in the electronic health record can change provider behavior and improve evidence-based care in a broad range of primary care clinics.
Clinicaltrials.gov ( NCT02534987 ).
临床预测规则(CPRs)是一种确定个体患者风险的方法,有助于医疗服务提供者在医疗现场做出更准确的决策。经过充分验证的CPRs未得到充分利用,但可能会减少急性呼吸道感染的抗生素过度使用。综合临床预测规则(iCPR)研究基于之前的一项单诊所研究,将两个CPRs整合到电子健康记录中,并评估其对医疗实践的影响。本文讨论了iCPR临床决策支持系统多中心整群随机对照试验的研究设计和实施,包括工具改编、可用性测试、人员培训以及在两个医疗系统的多个临床地点推广iCPR的实施研究。
iCPR工具基于两个经过充分验证的CPRs,一个用于链球菌性咽炎,一个用于肺炎。iCPR工具利用就诊原因触发风险计算器。医疗服务提供者完成风险计算器后会提供一个风险评分,该评分与一个医嘱集相关联。医嘱集指导循证医疗,包括病程记录文件、检查、处方药和患者指导。iCPR工具在与医疗服务提供者、医疗助理和诊所经理进行访谈以及两轮可用性测试的基础上进行了完善。使用模拟患者进行“近乎实时”的可用性测试,以确保iCPR符合医疗服务提供者的临床工作流程。在两个机构招募了33个家庭医学和普通内科初级保健诊所。诊所被随机分为接受关于链球菌性咽炎和肺炎诊断与治疗的学术详细指导(对照组)或接受学术详细指导并使用iCPR工具(干预组)。主要结局是干预组和对照组之间抗生素处方率的差异,次要结局是快速链球菌检测和胸部X光检查医嘱的差异。还将评估iCPR各组成部分的使用情况。
iCPR研究采用了强大的以用户为中心的设计,并基于之前的初步研究,以评估整合到电子健康记录中的CPRs是否能改变医疗服务提供者的行为,并在广泛的初级保健诊所中改善循证医疗。
Clinicaltrials.gov(NCT02534987)