Dellios Nikolaos, Teichgraeber Ulf, Chelaru Robert, Malich Ansgar, Papageorgiou Ismini E
Department of Experimental Radiology, Institute of Diagnostic and Interventional Radiology, Jena University Hospital, Friedrich-Schiller University, Jena, Germany; Institute of Radiology, Suedharz Hospital Nordhausen gGmbH, Nordhausen, Germany.
Department of Experimental Radiology, Institute of Diagnostic and Interventional Radiology, Jena University Hospital, Friedrich-Schiller University, Jena, Germany.
J Clin Imaging Sci. 2017 Feb 20;7:8. doi: 10.4103/jcis.JCIS_75_16. eCollection 2017.
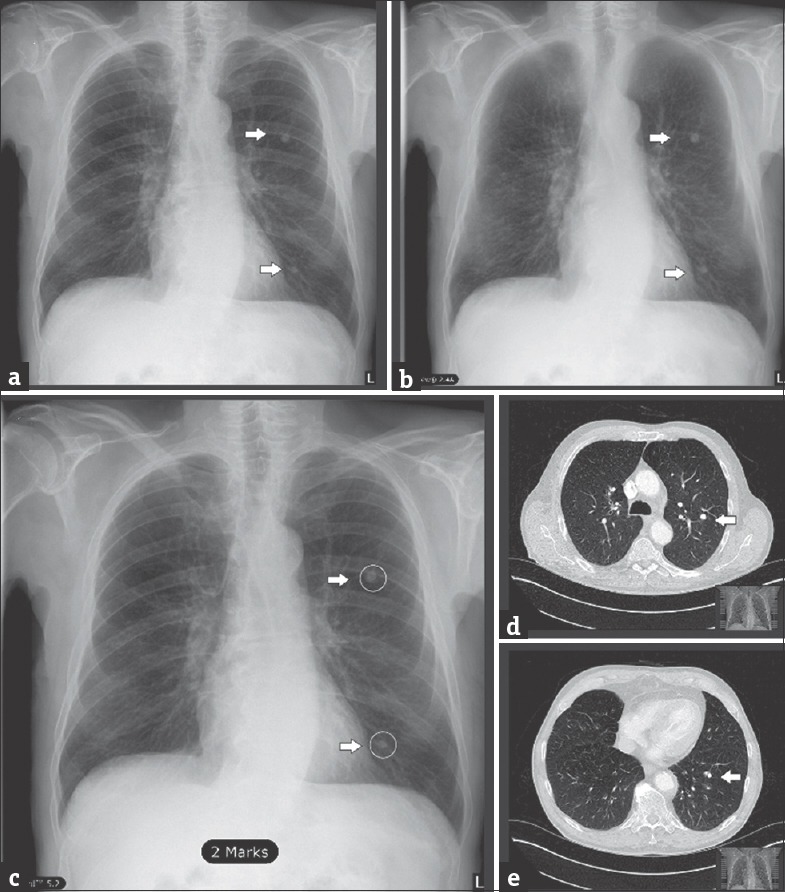
The most ubiquitous chest diagnostic method is the chest radiograph. A common radiographic finding, quite often incidental, is the nodular pulmonary lesion. The detection of small lesions out of complex parenchymal structure is a daily clinical challenge. In this study, we investigate the efficacy of the computer-aided detection (CAD) software package SoftView™ 2.4A for bone suppression and OnGuard™ 5.2 (Riverain Technologies, Miamisburg, OH, USA) for automated detection of pulmonary nodules in chest radiographs.
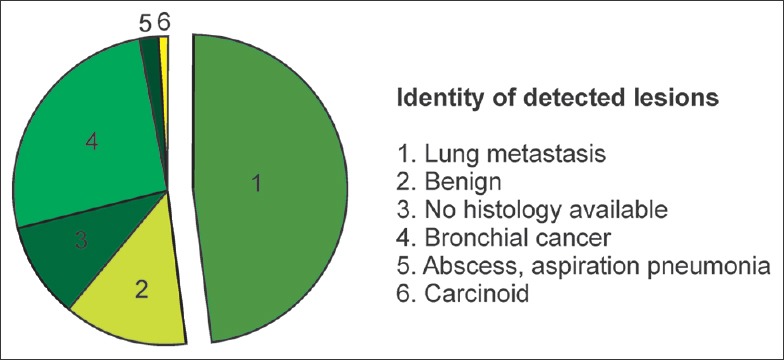
We retrospectively evaluated a dataset of 100 posteroanterior chest radiographs with pulmonary nodular lesions ranging from 5 to 85 mm. All nodules were confirmed with a consecutive computed tomography scan and histologically classified as 75% malignant. The number of detected lesions by observation in unprocessed images was compared to the number and dignity of CAD-detected lesions in bone-suppressed images (BSIs).
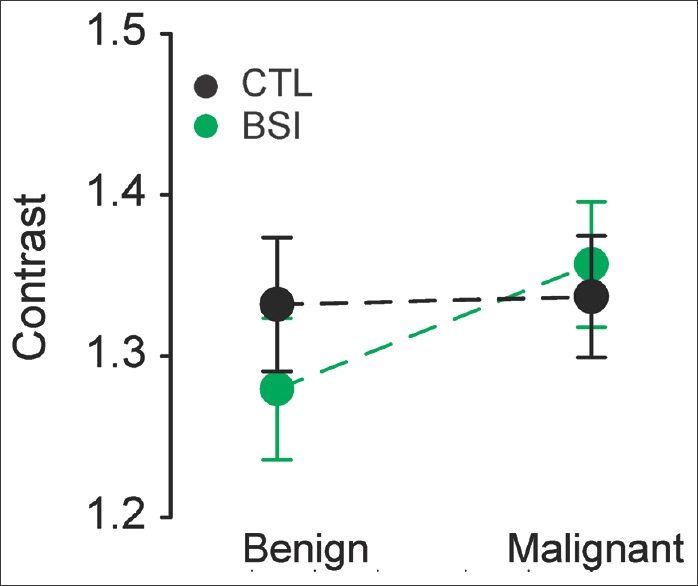
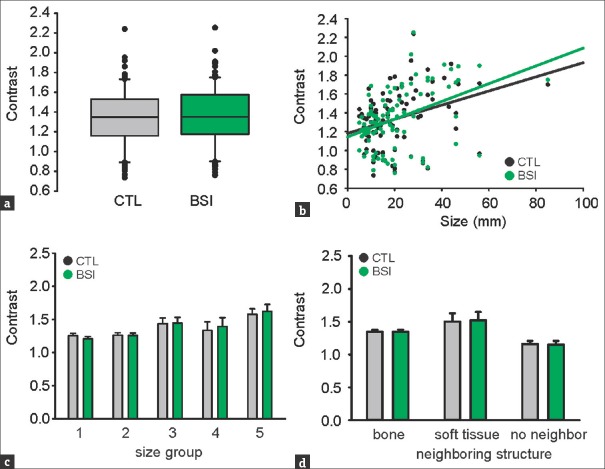
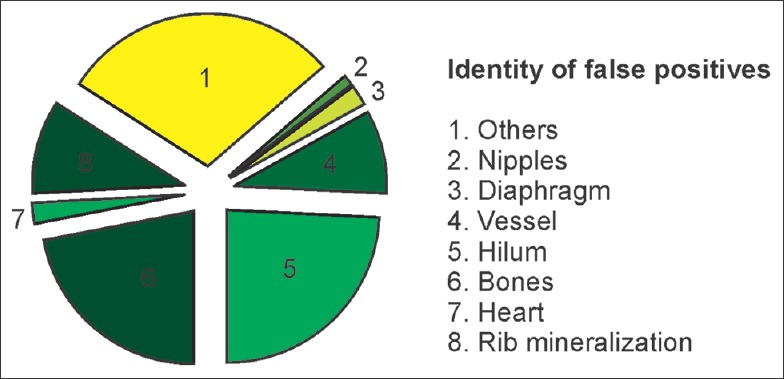
SoftView™ BSI does not affect the objective lesion-to-background contrast. OnGuard™ has a stand-alone sensitivity of 62% and specificity of 58% for nodular lesion detection in chest radiographs. The false positive rate is 0.88/image and the false negative (FN) rate is 0.35/image. From the true positive lesions, 20% were proven benign and 80% were malignant. FN lesions were 47% benign and 53% malignant.
We conclude that CAD does not qualify for a stand-alone standard of diagnosis. The use of CAD accompanied with a critical radiological assessment of the software suggested pattern appears more realistic. Accordingly, it is essential to focus on studies assessing the quality-time-cost profile of real-time (as opposed to retrospective) CAD implementation in clinical diagnostics.
最常用的胸部诊断方法是胸部X光片。一种常见的放射学表现,通常为偶然发现,是肺部结节性病变。从复杂的实质结构中检测小病变是日常临床挑战。在本研究中,我们调查了计算机辅助检测(CAD)软件包SoftView™ 2.4A用于骨抑制的效果以及OnGuard™ 5.2(Riverain Technologies,美国俄亥俄州米亚米斯堡)用于在胸部X光片中自动检测肺结节的效果。
我们回顾性评估了100例后前位胸部X光片的数据集,这些片子上有大小从5到85毫米的肺部结节性病变。所有结节均经连续计算机断层扫描确认,并经组织学分类,75%为恶性。将未处理图像中通过观察检测到的病变数量与骨抑制图像(BSIs)中CAD检测到的病变数量和特征进行比较。
SoftView™ BSI不影响目标病变与背景的对比度。OnGuard™在胸部X光片中检测结节性病变的独立灵敏度为62%,特异性为58%。假阳性率为0.88/图像,假阴性(FN)率为0.35/图像。在真阳性病变中,20%被证实为良性,80%为恶性。FN病变中47%为良性,53%为恶性。
我们得出结论,CAD不符合独立诊断标准。将CAD与对软件提示模式进行的严格放射学评估相结合使用似乎更符合实际。因此,必须专注于评估在临床诊断中实时(与回顾性相对)实施CAD的质量-时间-成本概况的研究。