Alosco Michael L, Duskin Jonathan, Besser Lilah M, Martin Brett, Chaisson Christine E, Gunstad John, Kowall Neil W, McKee Ann C, Stern Robert A, Tripodis Yorghos
Boston University Alzheimer's Disease and CTE Center, Boston University School of Medicine, Boston, MA, USA.
Department of Neurology, Boston University School of Medicine, Boston, MA, USA.
J Alzheimers Dis. 2017;57(3):953-968. doi: 10.3233/JAD-161205.
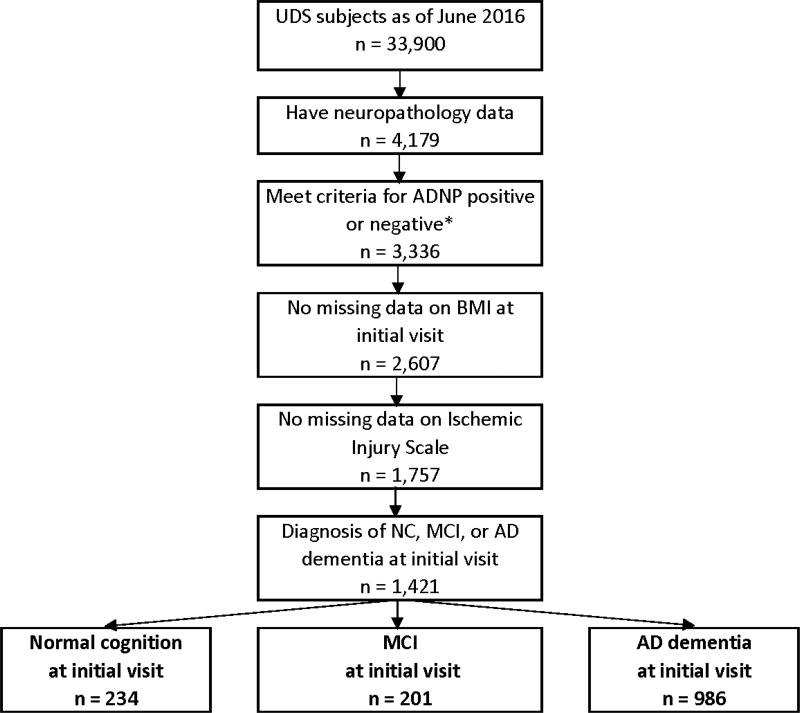
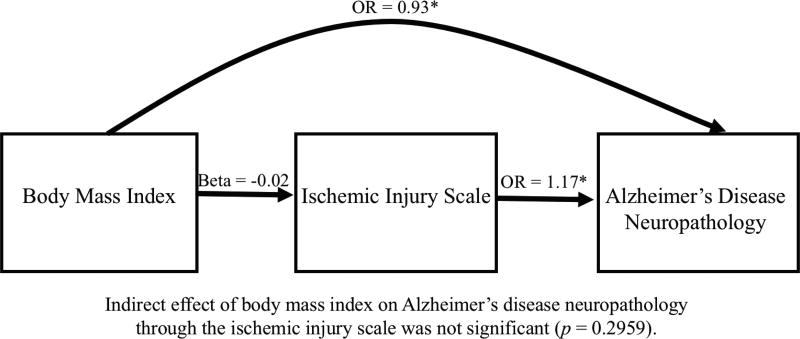
The relationship between late-life body mass index (BMI) and Alzheimer's disease (AD) is poorly understood due to the lack of research in samples with autopsy-confirmed AD neuropathology (ADNP). The role of cerebrovascular disease (CVD) in the interplay between late-life BMI and ADNP is unclear. We conducted a retrospective longitudinal investigation and used joint modeling of linear mixed effects to investigate causal relationships among repeated antemortem BMI measurements, CVD (quantified neuropathologically), and ADNP in an autopsy sample of subjects across the AD clinical continuum. The sample included 1,421 subjects from the National Alzheimer's Coordinating Center's Uniform Data Set and Neuropathology Data Set with diagnoses of normal cognition (NC; n = 234), mild cognitive impairment (MCI; n = 201), or AD dementia (n = 986). ADNP was defined as moderate to frequent neuritic plaques and Braak stageIII-VI. Ischemic Injury Scale (IIS) operationalized CVD. Joint modeling examined relationships among BMI, IIS, and ADNP in the overall sample and stratified by initial visit Clinical Dementia Rating score. Subject-specific random intercept for BMI was the predictor for ADNP due to minimal BMI change (p = 0.3028). Analyses controlling for demographic variables and APOE ɛ4 showed lower late-life BMI predicted increased odds of ADNP in the overall sample (p < 0.001), and in subjects with CDR of 0 (p = 0.0021) and 0.5 (p = 0.0012), but not ≥1.0 (p = 0.2012). Although higher IIS predicted greater odds of ADNP (p < 0.0001), BMI did not predict IIS (p = 0.2814). The current findings confirm lower late-life BMI confers increased odds for ADNP. Lower late-life BMI may be a preclinical indicator of underlying ADNP.
由于缺乏对经尸检确诊的阿尔茨海默病神经病理学(ADNP)样本的研究,人们对晚年体重指数(BMI)与阿尔茨海默病(AD)之间的关系了解甚少。脑血管疾病(CVD)在晚年BMI与ADNP相互作用中的作用尚不清楚。我们进行了一项回顾性纵向研究,并使用线性混合效应的联合模型来研究AD临床连续体中受试者尸检样本中生前重复BMI测量、CVD(通过神经病理学量化)和ADNP之间的因果关系。样本包括来自国家阿尔茨海默病协调中心统一数据集和神经病理学数据集的1421名受试者,他们被诊断为正常认知(NC;n = 234)、轻度认知障碍(MCI;n = 201)或AD痴呆(n = 986)。ADNP被定义为中度至频繁的神经炎性斑块和Braak III-VI期。缺血损伤量表(IIS)用于量化CVD。联合模型检查了总体样本中BMI、IIS和ADNP之间的关系,并按初次就诊临床痴呆评定量表评分进行分层。由于BMI变化极小(p = 0.3028),BMI的个体特异性随机截距是ADNP的预测因子。控制人口统计学变量和APOE ε4的分析表明,晚年较低的BMI预测了总体样本中ADNP几率的增加(p < 0.001),以及CDR为0(p = 0.0021)和0.5(p = 0.0012)的受试者中ADNP几率的增加,但在CDR≥1.0的受试者中未观察到(p = 0.2012)。虽然较高的IIS预测了ADNP的较高几率(p < 0.0001),但BMI并未预测IIS(p = 0.2814)。当前研究结果证实,晚年较低的BMI会增加ADNP的几率。晚年较低的BMI可能是潜在ADNP的临床前指标。