Maddur Mohan S, Stephen-Victor Emmanuel, Das Mrinmoy, Prakhar Praveen, Sharma Varun K, Singh Vikas, Rabin Magalie, Trinath Jamma, Balaji Kithiganahalli N, Bolgert Francis, Vallat Jean-Michel, Magy Laurent, Kaveri Srini V, Bayry Jagadeesh
Institut National de la Santé et de la Recherche Médicale, Unité 1138, Paris, 75006, France.
Centre de Recherche des Cordeliers, Equipe- Immunopathologie et immuno-intervention thérapeutique, Paris, 75006, France.
J Neuroinflammation. 2017 Mar 20;14(1):58. doi: 10.1186/s12974-017-0818-5.
Intravenous immunoglobulin (IVIG) is a polyspecific pooled immunoglobulin G preparation and one of the commonly used therapeutics for autoimmune diseases including those of neurological origin. A recent report in murine model proposed that IVIG expands regulatory T (T) cells via induction of interleukin 33 (IL-33). However, translational insight on these observations is lacking.
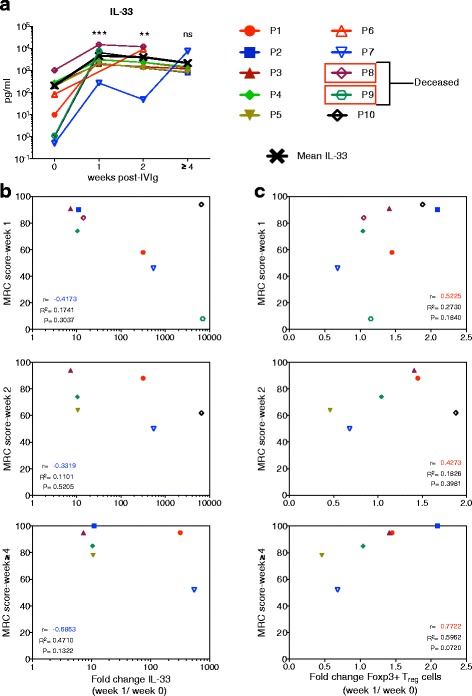
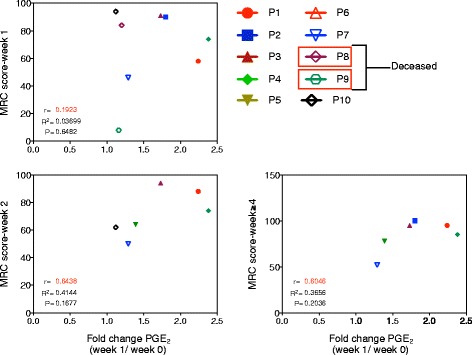
Ten newly diagnosed Guillain-Barré syndrome (GBS) patients were treated with IVIG at the rate of 0.4 g/kg for three to five consecutive days. Clinical evaluation for muscular weakness was performed by Medical Research Council (MRC) and modified Rankin scoring (MRS) system. Heparinized blood samples were collected before and 1, 2, and 4-5 weeks post-IVIG therapy. Peripheral blood mononuclear cells were stained for surface CD4 and intracellular Foxp3, IFN-γ, and tumor necrosis factor alpha (TNF-α) and were analyzed by flow cytometry. IL-33 and prostaglandin E2 in the plasma were measured by ELISA.
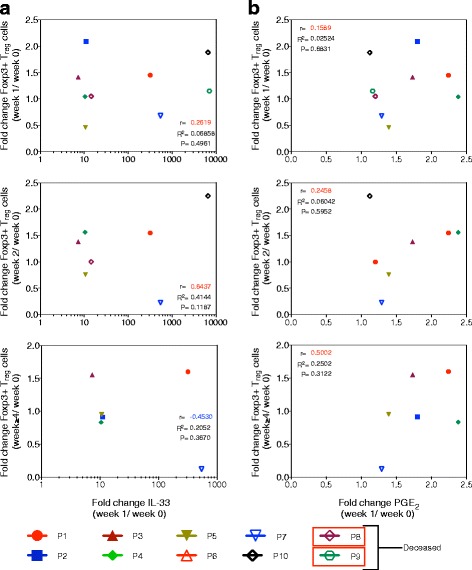
The fold changes in plasma IL-33 at week 1 showed no correlation with the MRC and MRS scores at weeks 1, 2, and ≥4 post-IVIG therapy. Clinical recovery following IVIG therapy appears to be associated with T cell response. Contrary to murine study, there was no association between the fold changes in IL-33 at week 1 and T cell frequency at weeks 1, 2, and ≥4 post-IVIG therapy. T cell-mediated clinical response to IVIG therapy in GBS patients was associated with reciprocal regulation of effector T cells-expressing TNF-α.
T cell expansion by IVIG in patients with autoimmune diseases lack correlation with IL-33. T cell frequency, but not plasma IL-33 levels, represents potential immunological biomarker to predict clinical response to IVIG therapy.
静脉注射免疫球蛋白(IVIG)是一种多特异性混合免疫球蛋白G制剂,是治疗自身免疫性疾病(包括神经源性自身免疫性疾病)的常用药物之一。最近在小鼠模型中的一份报告提出,IVIG通过诱导白细胞介素33(IL-33)来扩增调节性T(T)细胞。然而,缺乏对这些观察结果的转化性见解。
10例新诊断的吉兰-巴雷综合征(GBS)患者接受IVIG治疗,剂量为0.4 g/kg,连续三至五天。通过医学研究委员会(MRC)和改良Rankin评分(MRS)系统对肌无力进行临床评估。在IVIG治疗前以及治疗后1、2和4 - 5周采集肝素化血样。外周血单核细胞进行表面CD4以及细胞内Foxp3、干扰素-γ(IFN-γ)和肿瘤坏死因子α(TNF-α)染色,并通过流式细胞术进行分析。采用酶联免疫吸附测定法(ELISA)检测血浆中的IL-33和前列腺素E2。
第1周血浆IL-33的倍数变化与IVIG治疗后第1、2和≥4周的MRC和MRS评分均无相关性。IVIG治疗后的临床恢复似乎与T细胞反应相关。与小鼠研究相反,第1周IL-33的倍数变化与IVIG治疗后第1、2和≥4周的T细胞频率之间无关联。GBS患者对IVIG治疗的T细胞介导的临床反应与表达TNF-α的效应T细胞的相互调节有关。
自身免疫性疾病患者中IVIG诱导的T细胞扩增与IL-33缺乏相关性。T细胞频率而非血浆IL-33水平代表预测IVIG治疗临床反应的潜在免疫生物标志物。