Gelderblom Harald, Wüstenberg Torsten, McLean Tim, Mütze Lisanne, Fischer Wilhelm, Saft Carsten, Hoffmann Rainer, Süssmuth Sigurd, Schlattmann Peter, van Duijn Erik, Landwehrmeyer Bernhard, Priller Josef
Department of Neuropsychiatry, Charité-Universitätsmedizin Berlin, Berlin, Germany.
Department of Psychiatry, Charité-Universitätsmedizin Berlin, Berlin, Germany.
PLoS One. 2017 Mar 21;12(3):e0173872. doi: 10.1371/journal.pone.0173872. eCollection 2017.
To evaluate the efficacy and safety of bupropion in the treatment of apathy in Huntington's disease (HD).
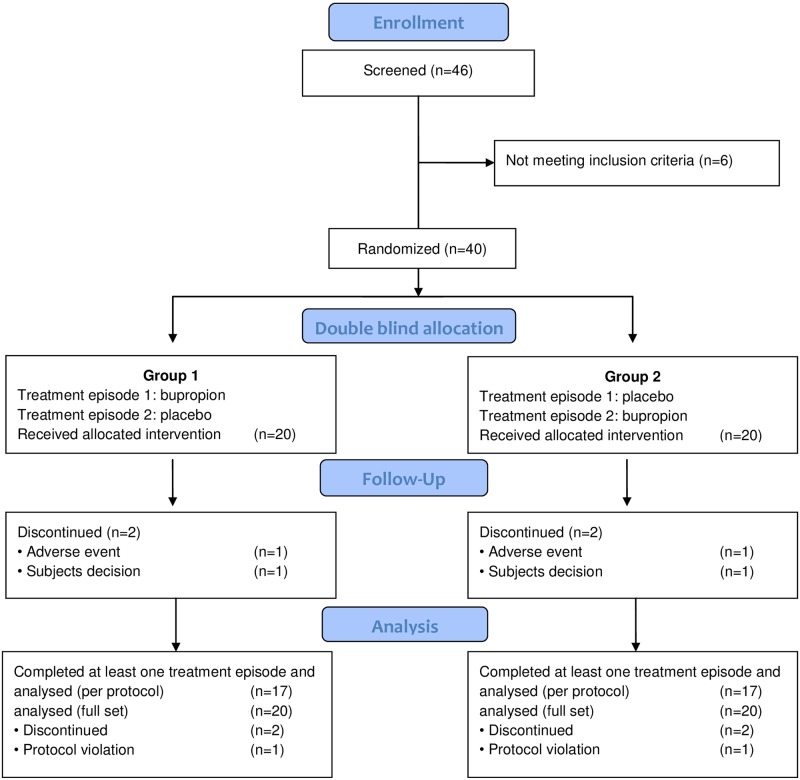
In this phase 2b multicentre, double-blind, placebo-controlled crossover trial, individuals with HD and clinical signs of apathy according to the Structured Clinical Interview for Apathy-Dementia (SCIA-D), but not depression (n = 40) were randomized to receive either bupropion 150/300mg or placebo daily for 10 weeks. The primary outcome parameter was a significant change of the Apathy Evaluation Scale (AES) score after ten weeks of treatment as judged by an informant (AES-I) living in close proximity with the study participant. The secondary outcome parameters included changes of 1. AES scores determined by the patient (AES-S) or the clinical investigator (AES-C), 2. psychiatric symptoms (NPI, HADS-SIS, UHDRS-Behavior), 3. cognitive performance (SDMT, Stroop, VFT, MMSE), 4. motor symptoms (UHDRS-Motor), 5. activities of daily function (TFC, UHDRS-Function), and 6. caregiver distress (NPI-D). In addition, we investigated the effect of bupropion on brain structure as well as brain responses and functional connectivity during reward processing in a gambling task using magnetic resonance imaging (MRI).
At baseline, there were no significant treatment group differences in the clinical primary and secondary outcome parameters. At endpoint, there was no statistically significant difference between treatment groups for all clinical primary and secondary outcome variables. Study participation, irrespective of the intervention, lessened symptoms of apathy according to the informant and the clinical investigator.
Bupropion does not alleviate apathy in HD. However, study participation/placebo effects were observed, which document the need for carefully controlled trials when investigating therapeutic interventions for the neuropsychiatric symptoms of HD.
ClinicalTrials.gov 01914965.
评估安非他酮治疗亨廷顿舞蹈症(HD)淡漠症状的疗效和安全性。
在这项2b期多中心、双盲、安慰剂对照交叉试验中,根据淡漠 - 痴呆结构化临床访谈(SCIA - D)有HD且有淡漠临床体征但无抑郁症状的个体(n = 40)被随机分为两组,分别每日服用150/300mg安非他酮或安慰剂,为期10周。主要结局参数是由与研究参与者密切生活的报告者(AES - I)判断的治疗10周后淡漠评估量表(AES)评分的显著变化。次要结局参数包括:1. 患者(AES - S)或临床研究者(AES - C)确定的AES评分变化;2. 精神症状(神经精神症状问卷、医院焦虑抑郁量表 - 自我评定量表、统一亨廷顿舞蹈病评定量表 - 行为部分);3. 认知表现(符号数字模式测验、斯特鲁普测验、言语流畅性测验、简易精神状态检查表);4. 运动症状(统一亨廷顿舞蹈病评定量表 - 运动部分);5. 日常功能活动(功能能力分类、统一亨廷顿舞蹈病评定量表 - 功能部分);6. 照料者痛苦程度(神经精神症状问卷 - 照料者版)。此外,我们使用磁共振成像(MRI)研究了安非他酮对大脑结构以及在赌博任务奖励处理过程中的大脑反应和功能连接的影响。
在基线时,临床主要和次要结局参数在治疗组之间无显著差异。在终点时,所有临床主要和次要结局变量在治疗组之间无统计学显著差异。无论干预措施如何,参与研究均减轻了报告者和临床研究者评估的淡漠症状。
安非他酮不能缓解HD的淡漠症状。然而,观察到了研究参与/安慰剂效应,这表明在研究HD神经精神症状的治疗干预措施时需要进行严格对照试验。
ClinicalTrials.gov 01914965。