van den Bosch Sven, Dijkema Tim, Kunze-Busch Martina C, Terhaard Chris H J, Raaijmakers Cornelis P J, Doornaert Patricia A H, Hoebers Frank J P, Vergeer Marije R, Kreike Bas, Wijers Oda B, Oyen Wim J G, Kaanders Johannes H A M
Department of radiation oncology, Radboud University Medical Center, huispost 874, P.O. Box 9101, Nijmegen, 6500, HB, The Netherlands.
Department of radiation oncology, University Medical Center Utrecht, Utrecht, The Netherlands.
BMC Cancer. 2017 Mar 21;17(1):208. doi: 10.1186/s12885-017-3195-7.
In definitive radiation therapy for head and neck cancer, clinically uninvolved cervical lymph nodes are irradiated with a so-called 'elective dose' in order to achieve control of clinically occult metastases. As a consequence of high-resolution diagnostic imaging, occult tumor volume has significantly decreased in the last decades. Since the elective dose is dependent on occult tumor volume, the currently used elective dose may be higher than necessary. Because bilateral irradiation of the neck contributes to dysphagia, xerostomia and hypothyroidism in a dose dependent way, dose de-escalation to these regions can open a window of opportunity to reduce toxicity and improve quality of life after treatment.
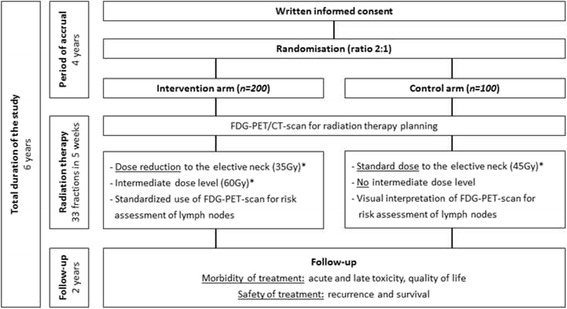
UPGRADE-RT is a multicenter, phase III, single-blinded, randomized controlled trial. Patients to be treated with definitive radiation therapy for a newly diagnosed stage T N M squamous cell carcinoma of the oropharynx, hypopharynx or larynx are eligible. Exclusion criteria are recurrent disease, oncologic surgery to the head and neck area, concomitant chemotherapy or epidermal growth factor receptor inhibitors. In total, 300 patients will be randomized in a 2:1 ratio to a treatment arm with or without de-escalation of the elective radiation dose and introduction of an intermediate dose-level for selected lymph nodes. Radiation therapy planning FDG-PET/CT-scans will be acquired to guide risk assessment of borderline-sized cervical nodes that can be treated with the intermediate dose level. Treatment will be given with intensity-modulated radiation therapy or volumetric arc therapy with simultaneous-integrated boost using an accelerated fractionation schedule, 33 fractions in 5 weeks. The primary endpoint is 'normalcy of diet' at 1 year after treatment (toxicity). The secondary endpoint is the actuarial rate of recurrence in electively irradiated lymph nodes at 2 years after treatment (safety).
The objective of the UPGRADE-RT trial is to investigate whether de-escalation of elective radiation dose and the introduction of an intermediate dose-level for borderline sized lymph nodes in the treatment of head and neck cancer will result in less radiation sequelae and improved quality of life after treatment without compromising the recurrence rate in the electively treated neck.
ClinicalTrials.gov Identifier: NCT02442375 .
在头颈部癌的根治性放射治疗中,对临床上未受累的颈部淋巴结给予所谓的“选择性剂量”照射,以实现对临床隐匿性转移灶的控制。由于高分辨率诊断成像技术的应用,在过去几十年中隐匿性肿瘤体积显著减小。由于选择性剂量取决于隐匿性肿瘤体积,目前使用的选择性剂量可能高于实际所需。由于颈部双侧照射会以剂量依赖的方式导致吞咽困难、口干和甲状腺功能减退,降低这些区域的照射剂量可以为降低治疗后的毒性和改善生活质量提供契机。
UPGRADE-RT是一项多中心、III期、单盲、随机对照试验。符合条件的患者为新诊断的口咽、下咽或喉鳞状细胞癌TₓNₓM₀期且接受根治性放射治疗的患者。排除标准为复发性疾病、头颈部区域的肿瘤手术、同步化疗或表皮生长因子受体抑制剂治疗。总共300名患者将按2:1的比例随机分为两组,一组接受选择性放射剂量降低并为选定淋巴结引入中间剂量水平的治疗方案,另一组不接受该方案。将获取放射治疗计划FDG-PET/CT扫描,以指导对可采用中间剂量水平治疗的临界大小颈部淋巴结的风险评估。治疗将采用调强放射治疗或容积弧形调强放疗,并使用加速分割方案同时进行增量照射,5周内照射33次。主要终点是治疗后1年的“饮食正常”(毒性)。次要终点是治疗后2年选择性照射淋巴结的精算复发率(安全性)。
UPGRADE-RT试验的目的是研究在头颈部癌治疗中降低选择性放射剂量并为临界大小淋巴结引入中间剂量水平是否会减少放射后遗症,改善治疗后的生活质量,同时不影响选择性治疗颈部的复发率。
ClinicalTrials.gov标识符:NCT02442375 。