Halliday Alice, Whitworth Hilary, Kottoor Sherine Hermagild, Niazi Umar, Menzies Sarah, Kunst Heinke, Bremang Samuel, Badhan Amarjit, Beverley Peter, Kon Onn Min, Lalvani Ajit
Tuberculosis Research Centre, Respiratory Medicine, National Heart and Lung Institute, Imperial College London, St Mary's Campus.
National Institute for Health Research, Health Protection Research Unit in Respiratory Infections, Imperial College London.
J Infect Dis. 2017 May 1;215(9):1480-1487. doi: 10.1093/infdis/jix107.
Recently acquired and remotely acquired latent Mycobacterium tuberculosis infection (LTBI) are clinically indistinguishable, yet recent acquisition of infection is the greatest risk factor for progression to tuberculosis in immunocompetent individuals. We aimed to evaluate the ability of cellular immune signatures that differ between active tuberculosis and LTBI to distinguish recently from remotely acquired LTBI.
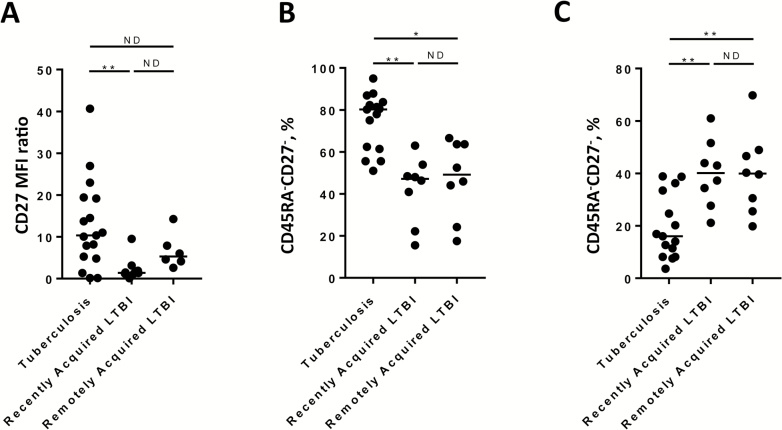
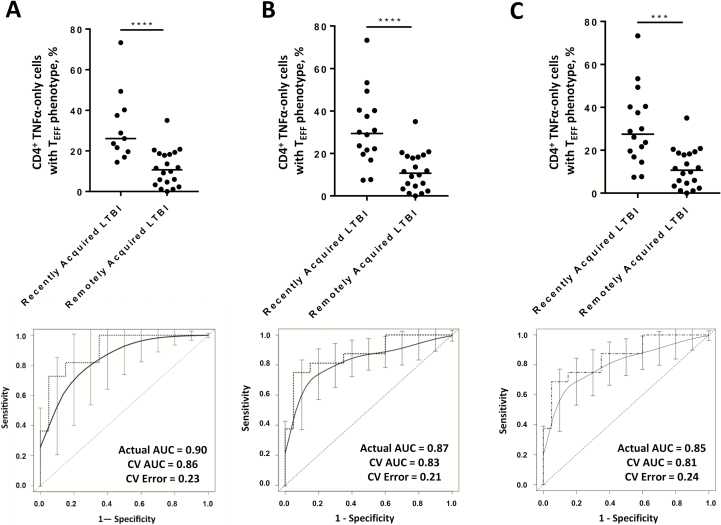
Fifty-nine individuals were recruited: 20 had active tuberculosis, 19 had recently acquired LTBI, and 20 had remotely acquired LTBI. The proportion of mycobacteria-specific CD4+ T cells secreting tumor necrosis factor α (TNF-α) but not interferon γ or interleukin 2 which had a differentiated effector phenotype (TNF-α-only TEFF), and the level of CD27 expression on IFN-γ-producing CD4+ T cells, were detected by flow cytometry.
The TNF-α-only TEFF signature was significantly higher in the group with recently acquired LTBI, compared with the group with remotely acquired LTBI (P < .0001), and it discriminated between these groups with high sensitivity and specificity, with an area under the curve of 0.87. Two signatures incorporating CD27 expression did not distinguish between recently and remotely acquired LTBI. Interestingly, the TNF-α-only TEFF signature in participants with recently acquired LTBI was more similar to that in participants with tuberculosis than that in participants with remotely acquired LTBI, suggesting that recently acquired LTBI is immunologically more similar to tuberculosis than remotely acquired LTBI.
These findings reveal marked biological heterogeneity underlying the clinically homogeneous phenotype of LTBI, providing a rationale for immunological risk stratification to improve targeting of LTBI treatment.
近期获得性潜伏性结核分枝杆菌感染(LTBI)和远程获得性潜伏性结核分枝杆菌感染在临床上难以区分,但在免疫功能正常的个体中,近期感染是进展为结核病的最大风险因素。我们旨在评估活动性结核病和LTBI之间不同的细胞免疫特征区分近期获得性与远程获得性LTBI的能力。
招募了59名个体:20例患有活动性结核病,19例患有近期获得性LTBI,20例患有远程获得性LTBI。通过流式细胞术检测分泌肿瘤坏死因子α(TNF-α)但不分泌干扰素γ或白细胞介素2的具有分化效应表型(仅TNF-α的TEFF)的分枝杆菌特异性CD4 + T细胞的比例,以及产生IFN-γ的CD4 + T细胞上CD27的表达水平。
与远程获得性LTBI组相比,近期获得性LTBI组中仅TNF-α的TEFF特征显著更高(P <.0001),并且它以高敏感性和特异性区分这些组,曲线下面积为0.87。包含CD27表达的两个特征不能区分近期获得性和远程获得性LTBI。有趣的是,近期获得性LTBI参与者中仅TNF-α的TEFF特征与结核病参与者中的特征比与远程获得性LTBI参与者中的特征更相似,这表明近期获得性LTBI在免疫学上比远程获得性LTBI更类似于结核病。
这些发现揭示了LTBI临床同质表型背后显著的生物学异质性,为免疫风险分层提供了理论依据,以改善LTBI治疗的靶向性。