Yeh Chi-Hsiao, Yu Hsiu-Chin, Huang Tzu-Yen, Huang Pin-Fu, Wang Yao-Chang, Chen Tzu-Ping, Yin Shun-Ying
Department of Thoracic and Cardiovascular Surgery, Chang Gung Memorial Hospital, 222 Mai-Chin Road, Keelung, 204, Taiwan, Republic of China.
College of Medicine, Chang Gung University, Tao-Yuan, Taiwan, Republic of China.
BMC Nephrol. 2017 Mar 22;18(1):99. doi: 10.1186/s12882-017-0514-9.
The variability of visit-to-visit (VVV) in systolic blood pressure (SBP) and diastolic blood pressure (DBP) is proved as a predictor of renal function deterioration in patients with non-diabetic chronic kidney disease. The purpose of this study was to investigate the relationship of the variability in SBP and the magnitude of renal function impairment for normal renal function patients in the first 10-years diagnosed with type II diabetes mellitus (DM).
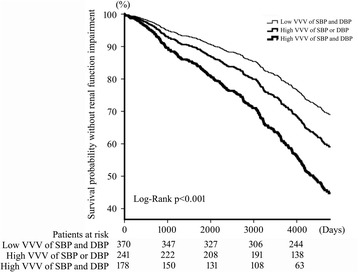
We retrospectively reviewed the electronic medical records of 789 patients who were first diagnosed with diabetes mellitus during 2000-2002 and regularly followed for 10 years with a total of 53,284 clinic visits. The stages of Chronic Kidney Disease (CKD) of every patient were determined using estimated glomerular filtration rate. The occurrence of nephropathy was defined in those patients whose CKD stages elevated equal or larger than three.
Patients were categorized according to the VVV of systolic and diastolic BP into three groups. Patients with high VVV of both SBP and DBP had a 2.44 fold (95% CI: 1.88-3.17, p < 0.001) increased risk of renal function impairment compared with patients with low VVV of both SBP and DBP. Risk of renal function impairment for patients with high VVV of either SBP or DBP had a 1.43-fold increase (95% CI: 1.08-1.89, p = 0.012) compared with patients with low VVV of both SBP and DBP. Cox regression analysis also demonstrated that every 1-year increase of DM diagnosed age significantly raised the risk of renal function impairment with a hazard ration of 1.05 (95% CI: 1.04-1.06, p < 0.001).
Not only VVV of SBP but also VVV in DBP is correlated with diabetic nephropathy in the first decade for patients diagnosed with type 2 DM.
就诊间收缩压(SBP)和舒张压(DBP)的变异性已被证明是预测非糖尿病慢性肾脏病患者肾功能恶化的指标。本研究旨在探讨初诊II型糖尿病(DM)10年内肾功能正常患者的SBP变异性与肾功能损害程度之间的关系。
我们回顾性分析了789例于2000年至2002年首次诊断为糖尿病且接受了10年定期随访、共53284次门诊就诊的患者的电子病历。使用估计的肾小球滤过率确定每位患者的慢性肾脏病(CKD)分期。肾病的发生定义为CKD分期升高等于或大于3期的患者。
根据SBP和DBP的就诊间变异性将患者分为三组。与SBP和DBP就诊间变异性均较低的患者相比,SBP和DBP就诊间变异性均较高的患者肾功能损害风险增加2.44倍(95%CI:1.88 - 3.17,p < 0.001)。与SBP和DBP就诊间变异性均较低的患者相比,SBP或DBP就诊间变异性较高的患者肾功能损害风险增加1.43倍(95%CI:1.08 - 1.89,p = 0.012)。Cox回归分析还表明,DM诊断年龄每增加1岁,肾功能损害风险显著增加,风险比为1.05(95%CI:1.04 - 1.06,p < 0.001)。
对于诊断为2型DM的患者,在最初十年中,不仅SBP的就诊间变异性,而且DBP的就诊间变异性均与糖尿病肾病相关。