Peng Hao, Chen Lei, Guo Rui, Zhang Yuan, Li Wen-Fei, Mao Yan-Ping, Sun Ying, Zhang Fan, Liu Li-Zhi, Tian Li, Ma Jun
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, 510060, Guangdong, P. R. China.
Department of Radiation Oncology, Sun Yat-sen University Cancer Center, Guangzhou, 510060, Guangdong, P. R. China.
Chin J Cancer. 2017 Mar 24;36(1):32. doi: 10.1186/s40880-017-0199-2.
Nasopharyngeal carcinoma (NPC) shows a high proportion of lymph node metastasis, and treatment guidelines have been developed for positive nodes. However, no irradiation guidelines have been proposed for patients with enlarged neck lymph nodes (ENLNs) that do not meet the radiological criteria of 10 mm in diameter for positive lymph nodes. This study aimed to determine the prognostic value and radiation dose for ENLNs in N0-category NPC patients treated with intensity-modulated radiotherapy (IMRT).
We reviewed the medical data of 251 patients with non-metastatic, N0-category NPC treated with IMRT. Receiver operating characteristic curves were used to calculate the cut-off value of the ENLN diameter for the prediction of disease failure. The biological equivalent dose (BED) for ENLNs was calculated. Patient survival was compared between the small and large ENLN groups. Independent prognostic factors were identified using the Cox proportional hazards model.
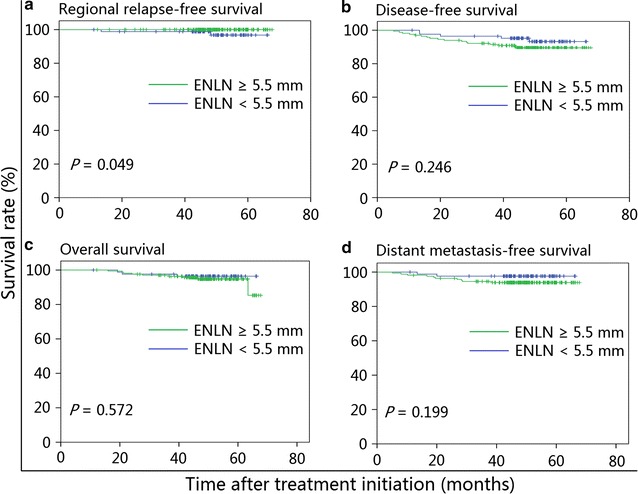
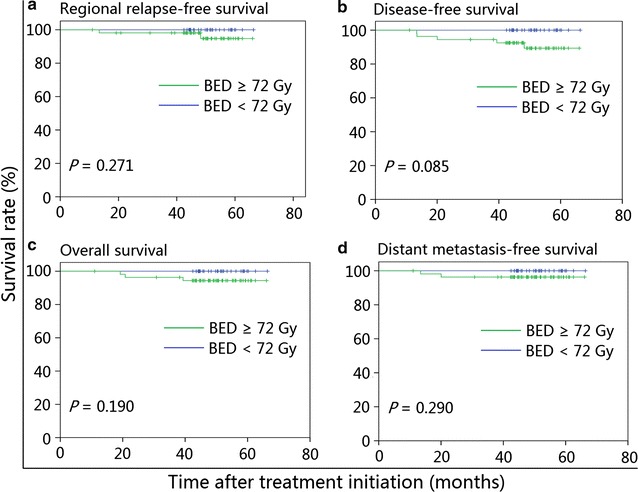
The estimated 4-year regional relapse-free survival rate was higher in patients with ENLNs ≥5.5 mm than in those with ENLNs <5.5 mm (100% vs. 98.8%, P = 0.049), whereas disease-free, overall, and distant metastasis-free survival rates were similar between the two groups. After adjusting for various factors, ENLN diameter was not identified as an independent prognostic factor (P > 0.05 for all survival rates). In the subgroup analysis, patients receiving BED ≥72 Gy had a similar prognosis as patients receiving BED <72 Gy in both the small and large ENLN groups. The multivariate analysis also confirmed that BED ≥72 Gy was not associated with significantly improved prognosis in patients with N0-category NPC.
A BED of 72 Gy to ENLNs is considerably sufficient to provide a clinical benefit to patients with N0-category NPC. Prospective studies are warranted to validate the findings in the present study.
鼻咽癌(NPC)的淋巴结转移比例较高,针对阳性淋巴结已制定了治疗指南。然而,对于颈部淋巴结肿大(ENLNs)但未达到阳性淋巴结直径10毫米放射学标准的患者,尚未提出照射指南。本研究旨在确定调强放疗(IMRT)治疗的N0期NPC患者中ENLNs的预后价值和放射剂量。
我们回顾了251例接受IMRT治疗的非转移性N0期NPC患者的医疗数据。采用受试者操作特征曲线计算ENLN直径的截断值,以预测疾病失败。计算ENLNs的生物等效剂量(BED)。比较小和大ENLN组患者的生存情况。使用Cox比例风险模型确定独立预后因素。
ENLNs≥5.5毫米的患者4年区域无复发生存率估计高于ENLNs<5.5毫米的患者(100%对98.8%,P = 0.049),而两组间无病生存、总生存和远处转移无病生存率相似。在调整各种因素后,ENLN直径未被确定为独立预后因素(所有生存率P>0.05)。在亚组分析中,小和大ENLN组中接受BED≥72 Gy的患者与接受BED<72 Gy的患者预后相似。多变量分析也证实,BED≥72 Gy与N0期NPC患者预后显著改善无关。
ENLNs的BED为72 Gy足以使N0期NPC患者获得临床益处。有必要进行前瞻性研究以验证本研究结果。