Mao Yan-Ping, Tang Ling-Long, Chen Lei, Sun Ying, Qi Zhen-Yu, Zhou Guan-Qun, Liu Li-Zhi, Li Li, Lin Ai-Hua, Ma Jun
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, 510060, Guangdong, P. R. China.
Department of Radiation Oncology, Sun Yat-sen University Cancer Center, Guangzhou, 510060, Guangdong, P. R. China.
Chin J Cancer. 2016 Dec 28;35(1):103. doi: 10.1186/s40880-016-0167-2.
The prognostic values of staging parameters require continual re-assessment amid changes in diagnostic and therapeutic methods. This study aimed to identify the prognostic factors and failure patterns of non-metastatic nasopharyngeal carcinoma (NPC) in the intensity-modulated radiotherapy (IMRT) era.
We reviewed the data from 749 patients with newly diagnosed, biopsy-proven, non-metastatic NPC in our cancer center (South China, an NPC endemic area) between January 2003 and December 2007. All patients underwent magnetic resonance imaging (MRI) before receiving IMRT. The actuarial survival rates were estimated using the Kaplan-Meier method, and survival curves were compared using the log-rank test. Multivariate analyses with the Cox proportional hazards model were used to test for the independent prognostic factors by backward eliminating insignificant explanatory variables.
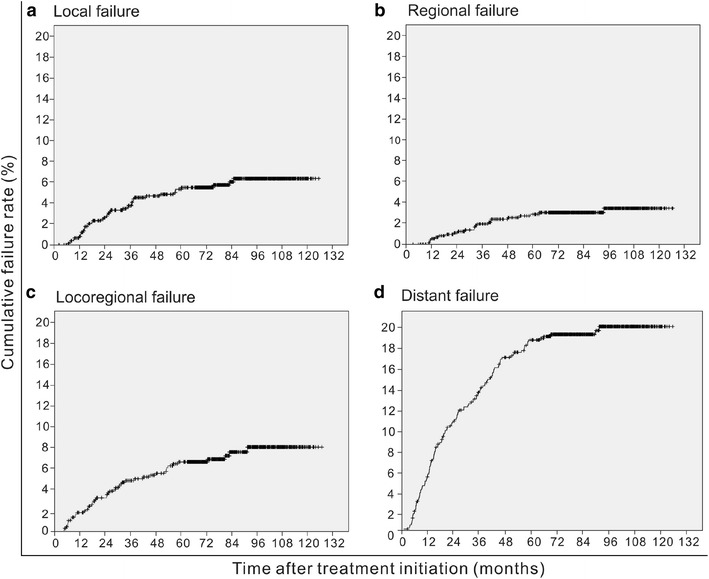
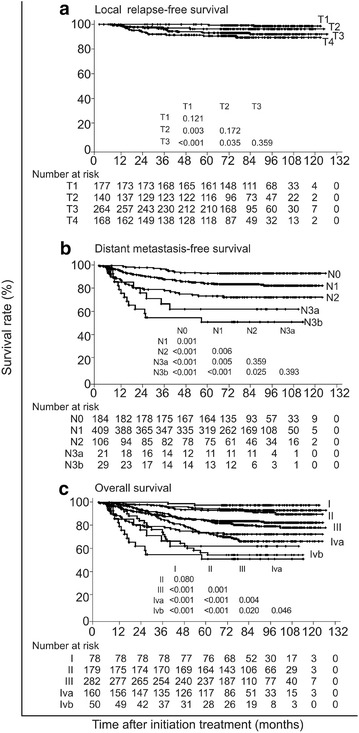
The 5-year occurrence rates of local failure, regional failure, locoregional failure, and distant failure were 5.4, 3.0, 7.4, and 17.4%, respectively. The 5-year survival rates were as follows: local relapse-free survival, 94.6%; nodal relapse-free survival, 97.0%; distant metastasis-free survival, 82.6%; disease-free survival, 75.1%; and overall survival, 82.0%. Multivariate Cox regression analysis revealed that orbit involvement was the only significant prognostic factor for local failure (P = 0.011). Parapharyngeal tumor extension, retropharyngeal lymph node involvement, and the laterality, longest diameter, and Ho's location of the cervical lymph nodes were significant prognostic factors for both distant failure and disease failure (all P < 0.05). Intracranial extension had significant prognostic value for distant failure (P = 0.040).
The key failure pattern for NPC was distant metastasis in the IMRT era. With changes in diagnostic and therapeutic technologies as well as treatment modalities, the significant prognostic parameters for local control have also been altered substantially.
在诊断和治疗方法不断变化的情况下,分期参数的预后价值需要持续重新评估。本研究旨在确定调强放疗(IMRT)时代非转移性鼻咽癌(NPC)的预后因素和失败模式。
我们回顾了2003年1月至2007年12月期间在我们癌症中心(中国南方,鼻咽癌高发地区)新诊断、经活检证实的749例非转移性NPC患者的数据。所有患者在接受IMRT之前均接受了磁共振成像(MRI)检查。采用Kaplan-Meier方法估计精算生存率,并使用对数秩检验比较生存曲线。使用Cox比例风险模型进行多变量分析,通过向后消除无显著意义的解释变量来检验独立预后因素。
局部失败、区域失败、局部区域失败和远处失败的5年发生率分别为5.4%、3.0%、7.4%和17.4%。5年生存率如下:局部无复发生存率为94.6%;淋巴结无复发生存率为97.0%;无远处转移生存率为82.6%;无病生存率为75.1%;总生存率为82.0%。多变量Cox回归分析显示,眼眶受累是局部失败的唯一显著预后因素(P = 0.011)。咽旁肿瘤扩展、咽后淋巴结受累以及颈部淋巴结的侧别、最长径和何杰金氏病位置是远处失败和疾病失败的显著预后因素(所有P < 0.05)。颅内扩展对远处失败具有显著预后价值(P = 0.040)。
在IMRT时代,NPC的关键失败模式是远处转移。随着诊断和治疗技术以及治疗方式的变化,局部控制的显著预后参数也发生了很大改变。