Naessens James M, Van Such Monica B, Nesse Robert E, Dilling James A, Swensen Stephen J, Thompson Kristine M, Orlowski Janis M, Santrach Paula J
J.M. Naessens is professor of health services research, Mayo Clinic, and scientific director, Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Jacksonville, Florida. M.B. Van Such is principal analyst, Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, Minnesota. R.E. Nesse is senior medical director for payment reform and professor of family medicine, Mayo Clinic, Rochester, Minnesota. J.A. Dilling is chief operating officer for quality, Baylor, Scott & White Health, Dallas, Texas. S.J. Swensen is professor of radiology and past director of quality, Mayo Clinic, Rochester, Minnesota. K.M. Thompson is assistant professor of emergency medicine and performance improvement officer, Mayo Clinic, Jacksonville, Florida. J.M. Orlowski is chief health care officer, Association of American Medical Colleges, Washington, DC. P.J. Santrach is associate professor of laboratory medicine and pathology and chief quality officer, Mayo Clinic, Rochester, Minnesota.
Acad Med. 2017 Jul;92(7):943-950. doi: 10.1097/ACM.0000000000001654.
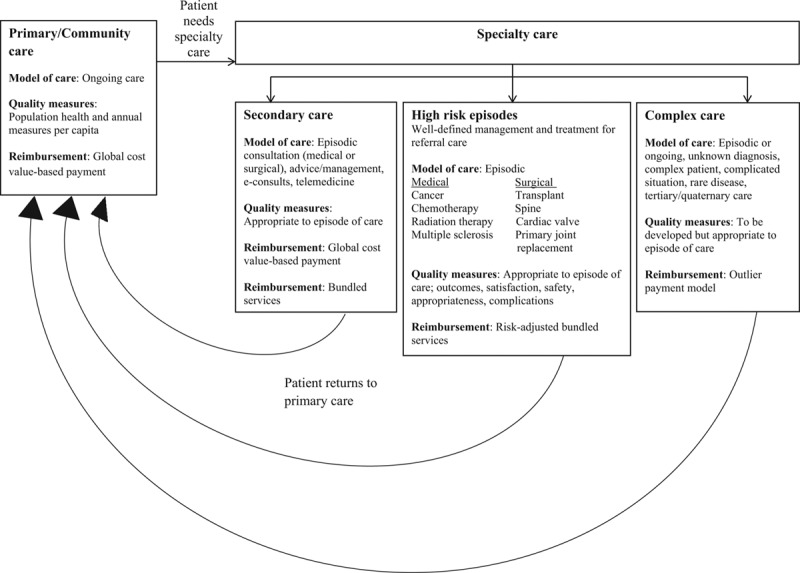
The majority of quality measures used to assess providers and hospitals are based on easily obtained data, focused on a few dimensions of quality, and developed mainly for primary/community care and population health. While this approach supports efforts focused on addressing the triple aim of health care, many current quality report cards and assessments do not reflect the breadth or complexity of many referral center practices.In this article, the authors highlight the differences between population health efforts and referral care and address issues related to value measurement and performance assessment. They discuss why measures may need to differ across the three levels of care (primary/community care, secondary care, complex care) and illustrate the need for further risk adjustment to eliminate referral bias.With continued movement toward value-based purchasing, performance measures and reimbursement schemes need to reflect the increased level of intensity required to provide complex care. The authors propose a framework to operationalize value measurement and payment for specialty care, and they make specific recommendations to improve performance measurement for complex patients. Implementing such a framework to differentiate performance measures by level of care involves coordinated efforts to change both policy and operational platforms. An essential component of this framework is a new model that defines the characteristics of patients who require complex care and standardizes metrics that incorporate those definitions.
用于评估医疗服务提供者和医院的大多数质量指标是基于容易获取的数据,聚焦于质量的几个维度,并且主要是为初级/社区医疗和人群健康而制定的。虽然这种方法有助于实现以医疗保健的三重目标为重点的努力,但许多当前的质量报告卡和评估并未反映出许多转诊中心业务的广度或复杂性。在本文中,作者强调了人群健康工作与转诊护理之间的差异,并探讨了与价值衡量和绩效评估相关的问题。他们讨论了为什么不同级别的护理(初级/社区护理、二级护理、复杂护理)可能需要不同的指标,并说明了进一步进行风险调整以消除转诊偏差的必要性。随着向基于价值的采购的持续推进,绩效指标和报销方案需要反映出提供复杂护理所需的更高强度水平。作者提出了一个框架,用于实施专科护理的价值衡量和支付,并针对改善复杂患者的绩效衡量提出了具体建议。实施这样一个按护理级别区分绩效指标的框架需要协调努力,以改变政策和运营平台。该框架的一个重要组成部分是一个新模型,该模型定义了需要复杂护理的患者的特征,并标准化纳入这些定义的指标。