Mikami Maya, Zhang Yi, Kim Benjamin, Worgall Tilla S, Groeben Harald, Emala Charles W
Department of Anesthesiology, College of Physicians and Surgeons of Columbia University, 630 West 168th Street, P&S Box 46, New York, NY, 10032, USA.
Department of Pathology and Cell Biology, College of Physicians and Surgeons of Columbia University, New York, NY, USA.
BMC Anesthesiol. 2017 Mar 29;17(1):52. doi: 10.1186/s12871-017-0345-z.
Airway instrumentation can evoke upper airway reflexes including bronchoconstriction and cough which can cause serious complications including airway trauma, laryngospasm or bronchospasm which may in turn lead to difficulty with ventilation and hypoxemia. These airway events are mediated in part by irritant-induced neuronal modulation of airway tone and cough responses. We investigated whether the commonly used anesthetic agents dexmedetomidine, lidocaine or remifentanil attenuated neuronal and airway smooth muscle responses in the upper airways of guinea pigs.
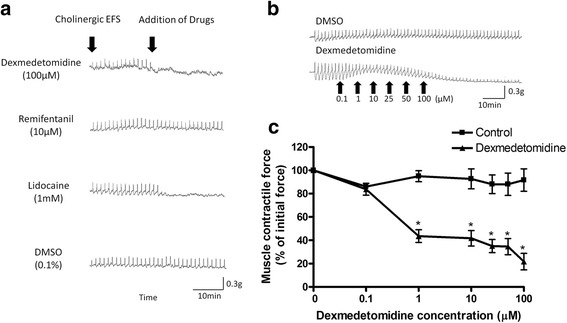
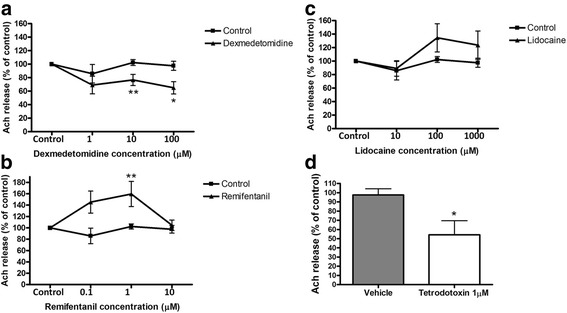
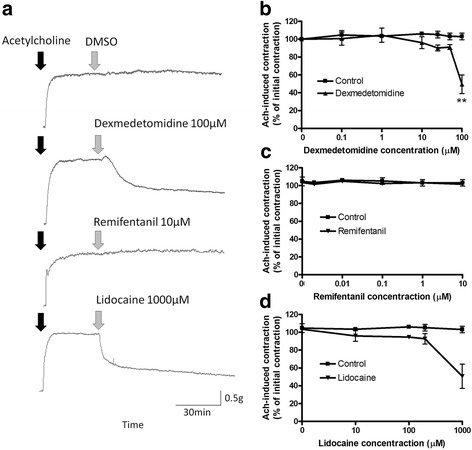
The ability of dexmedetomidine, lidocaine or remifentanil to attenuate direct cholinergic nerve stimulation, C-fiber stimulation or direct smooth muscle contraction were studied using isolated tracheal rings from male guinea pigs under four paradigms; (1) the magnitude of contractile force elicited by cholinergic electrical field stimulation (EFS); (2) the amount of acetylcholine released during cholinergic EFS; (3) the direct airway smooth muscle relaxation of a sustained acetylcholine-induced contraction and (4) the magnitude of C-fiber mediated contraction.
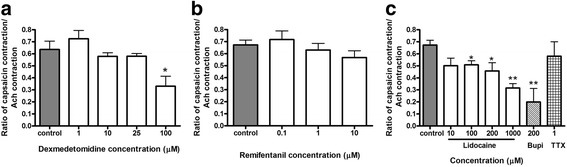
Dexmedetomidine (1-100 μM) and lidocaine (1 mM) attenuated cholinergic 30Hz EFS-induced tracheal ring contraction while remifentanil (10 μM) had no effect. Dexmedetomidine at 10 μM (p = 0.0047) and 100 μM (p = 0.01) reduced cholinergic EFS-induced acetylcholine release while lidocaine (10 μM-1 mM) and remifentanil (0.1-10 μM) did not. Tracheal ring muscle force induced by the exogenous addition of the contractile agonist acetylcholine or by a prototypical C-fiber analogue of capsaicin were also attenuated by 100 μM dexmedetomidine (p = 0.0061 and p = 0.01, respectively). The actual tracheal tissue concentrations of dexmedetomidine achieved (0.54-26 nM) following buffer application of 1-100 μM of dexmedetomidine were within the range of clinically achieved plasma concentrations (12 nM).
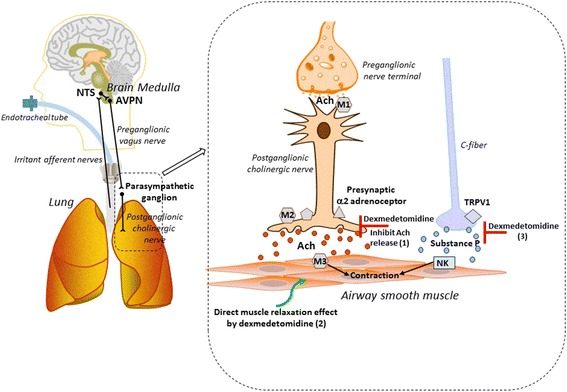
The α2 adrenoceptor agonist dexmedetomidine reduced cholinergic EFS-induced contractions and acetylcholine release consistent with the presence of inhibitory α2 adrenoceptors on the prejunctional side of the postganglionic cholinergic nerve-smooth muscle junction. Dexmedetomidine also attenuated both exogenous acetylcholine-induced contraction and C-fiber mediated contraction, suggesting a direct airway smooth muscle effect and an underlying mechanism for cough suppression, respectively.
气道器械操作可诱发上呼吸道反射,包括支气管收缩和咳嗽,这可能导致严重并发症,如气道创伤、喉痉挛或支气管痉挛,进而可能导致通气困难和低氧血症。这些气道事件部分是由刺激物诱导的气道张力和咳嗽反应的神经元调节介导的。我们研究了常用麻醉剂右美托咪定、利多卡因或瑞芬太尼是否能减弱豚鼠上呼吸道的神经元和气道平滑肌反应。
在四种模式下,使用雄性豚鼠的离体气管环研究右美托咪定、利多卡因或瑞芬太尼减弱直接胆碱能神经刺激、C纤维刺激或直接平滑肌收缩的能力;(1)胆碱能电场刺激(EFS)引起的收缩力大小;(2)胆碱能EFS期间释放的乙酰胆碱量;(3)持续乙酰胆碱诱导收缩的直接气道平滑肌松弛;(4)C纤维介导收缩的大小。
右美托咪定(1-100μM)和利多卡因(1mM)减弱了胆碱能30Hz EFS诱导的气管环收缩,而瑞芬太尼(10μM)无作用。10μM(p = 0.0047)和100μM(p = 0.01)的右美托咪定减少了胆碱能EFS诱导的乙酰胆碱释放,而利多卡因(10μM-1mM)和瑞芬太尼(0.1-10μM)则没有。外源性添加收缩激动剂乙酰胆碱或辣椒素的典型C纤维类似物诱导的气管环肌力也被100μM右美托咪定减弱(分别为p = 0.0061和p = 0.01)。在缓冲液中应用1-100μM右美托咪定后实际达到的气管组织浓度(0.54-26 nM)在临床达到的血浆浓度范围内(12 nM)。
α2肾上腺素能受体激动剂右美托咪定降低了胆碱能EFS诱导的收缩和乙酰胆碱释放,这与节后胆碱能神经-平滑肌接头节前侧存在抑制性α2肾上腺素能受体一致(此处存在抑制性α2肾上腺素能受体,所以右美托咪定降低了胆碱能EFS诱导的收缩和乙酰胆碱释放)。右美托咪定还减弱了外源性乙酰胆碱诱导的收缩和C纤维介导的收缩,分别提示了直接的气道平滑肌效应和咳嗽抑制的潜在机制。