Gleeson Sarah, Liao Yi-Wen, Dugo Clementina, Cave Andrew, Zhou Lifeng, Ayar Zina, Christiansen Jonathan, Scott Tony, Dawson Liane, Gavin Andrew, Schlegel Todd T, Gladding Patrick
Department of Cardiology, North Shore Hospital, Waitemata District Health Board, Auckland, New Zealand.
Division of Cardiology, Azienda Ospedaliera Universitaria Integrata, Verona, Italy.
PLoS One. 2017 Mar 30;12(3):e0171069. doi: 10.1371/journal.pone.0171069. eCollection 2017.
Increased spatial QRS-T angle has been shown to predict appropriate implantable cardioverter defibrilIator (ICD) therapy in patients with left ventricular systolic dysfunction (LVSD). We performed a retrospective cohort study in patients with left ventricular ejection fraction (LVEF) 31-40% to assess the relationship between the spatial QRS-T angle and other advanced ECG (A-ECG) as well as echocardiographic metadata, with all-cause mortality or ICD implantation for secondary prevention.
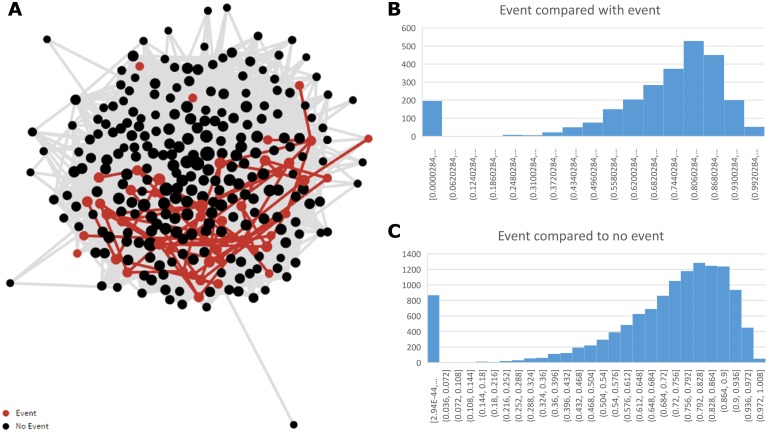
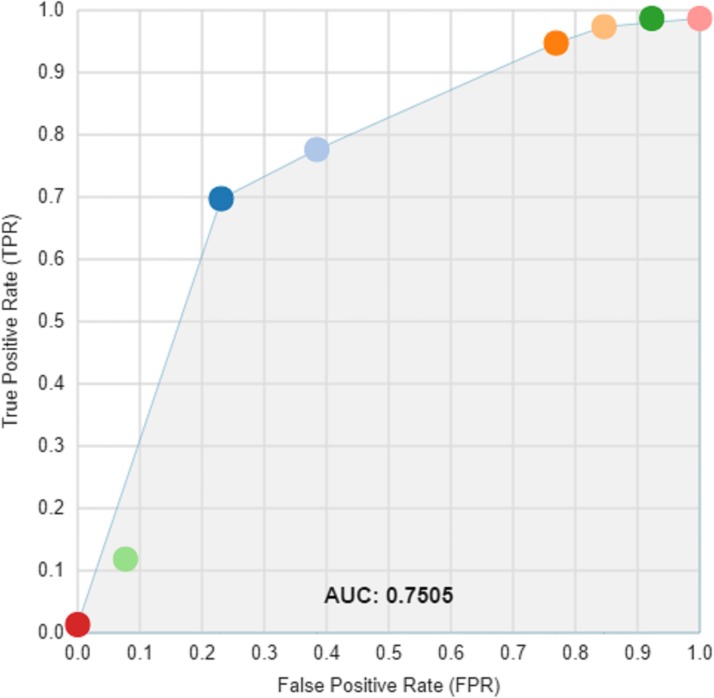
534 patients ≤75 years of age with LVEF 31-40% were identified through an echocardiography reporting database. Digital 12-lead ECGs were retrospectively matched to 295 of these patients, for whom echocardiographic and A-ECG metadata were then generated. Data mining was applied to discover novel ECG and echocardiographic markers of risk. Machine learning was used to develop a model to predict possible outcomes.
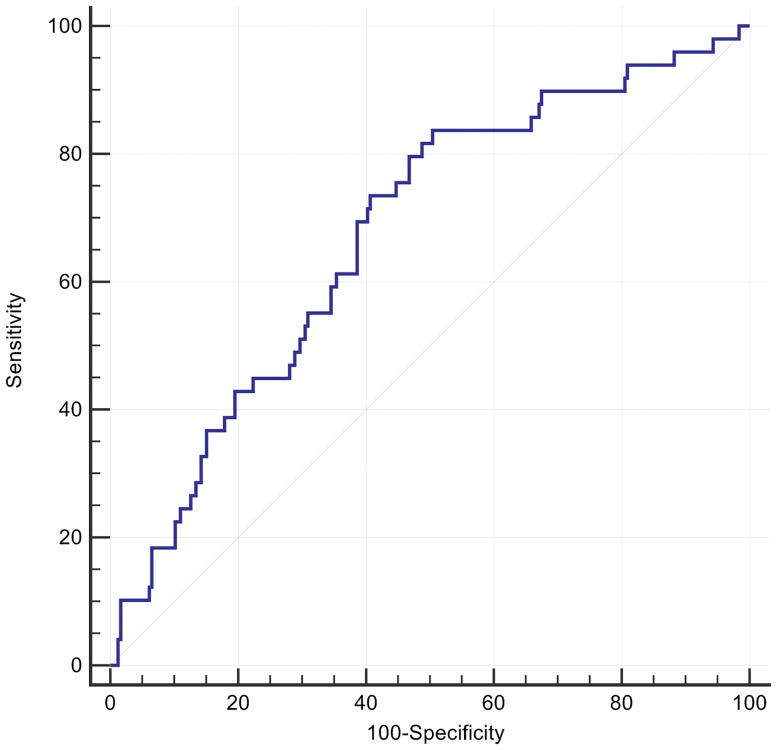
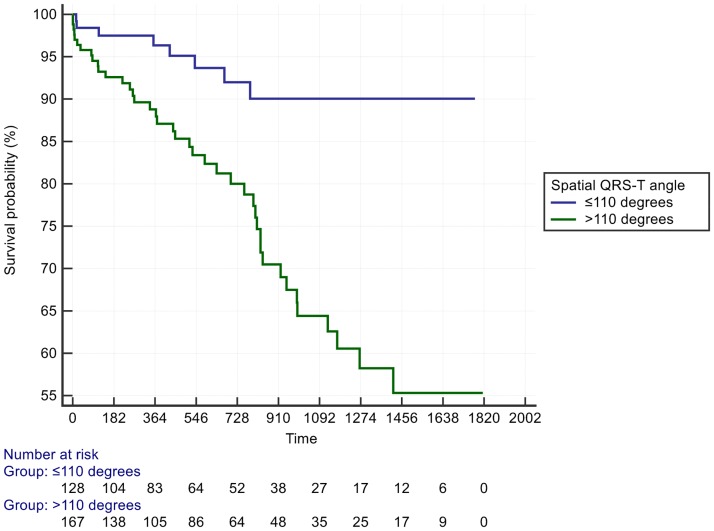
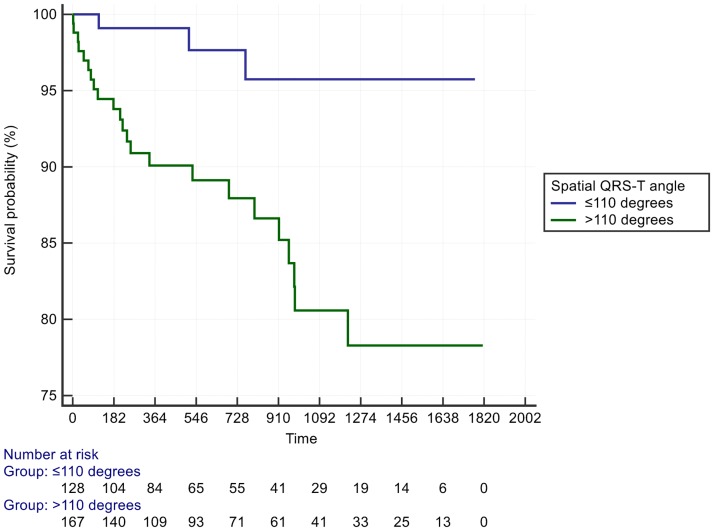
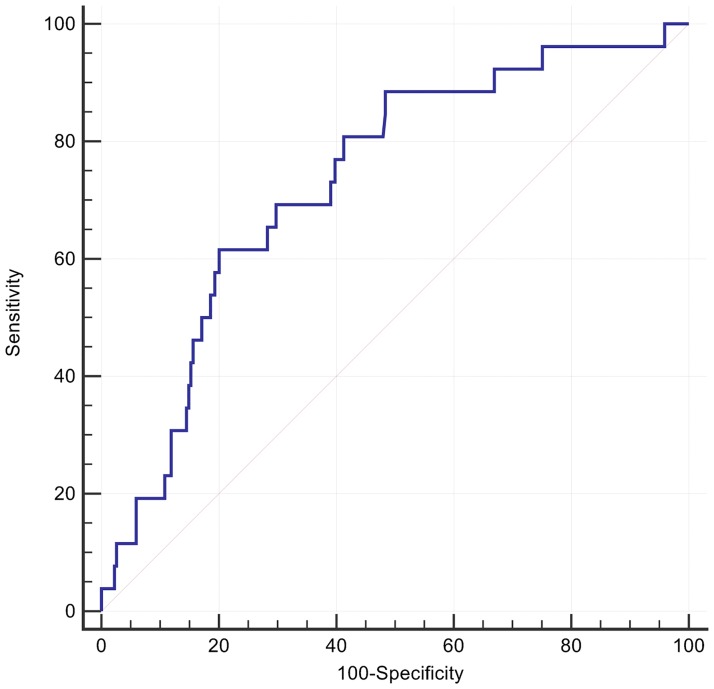
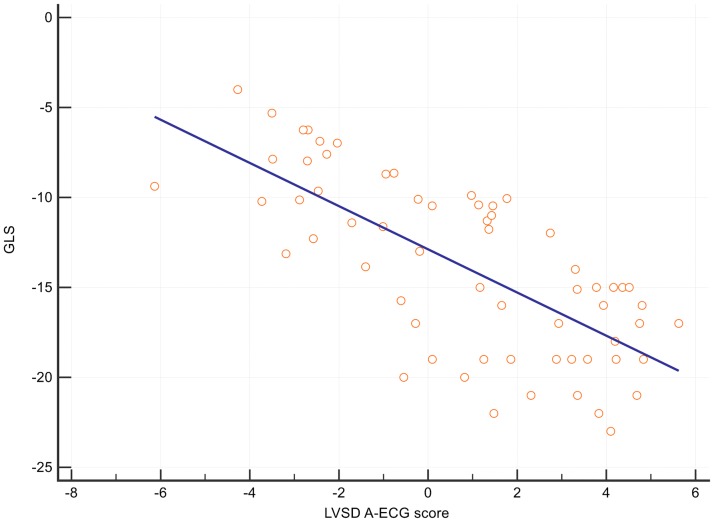
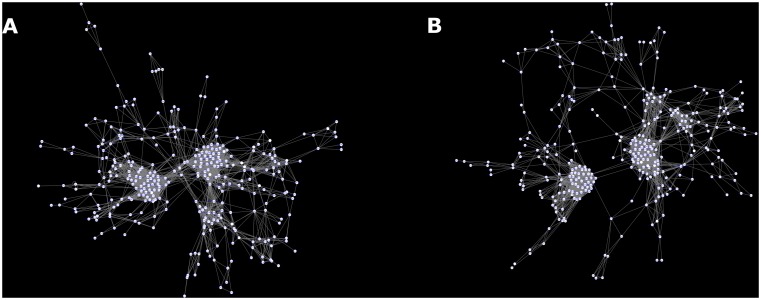
49 patients (17%) had events, defined as either mortality (n = 16) or ICD implantation for secondary prevention (n = 33). 72 parameters (58 A-ECG, 14 echocardiographic) were univariately different (p<0.05) in those with vs. without events. After adjustment for multiplicity, 24 A-ECG parameters and 3 echocardiographic parameters remained different (p<2x10-3). These included the posterior-to-leftward QRS loop ratio from the derived vectorcardiographic horizontal plane (previously associated with pulmonary artery pressure, p = 2x10-6); spatial mean QRS-T angle (134 vs. 112°, p = 1.6x10-4); various repolarisation vectors; and a previously described 5-parameter A-ECG score for LVSD (p = 4x10-6) that also correlated with echocardiographic global longitudinal strain (R2 = - 0.51, P < 0.0001). A spatial QRS-T angle >110° had an adjusted HR of 3.4 (95% CI 1.6 to 7.4) for secondary ICD implantation or all-cause death and adjusted HR of 4.1 (95% CI 1.2 to 13.9) for future heart failure admission. There was a loss of complexity between A-ECG and echocardiographic variables with an increasing degree of disease.
Spatial QRS-T angle >110° was strongly associated with arrhythmic events and all-cause death. Deep analysis of global ECG and echocardiographic metadata revealed underlying relationships, which otherwise would not have been appreciated. Delivered at scale such techniques may prove useful in clinical decision making in the future.
空间QRS-T角增大已被证明可预测左心室收缩功能障碍(LVSD)患者植入式心律转复除颤器(ICD)的合理治疗。我们对左心室射血分数(LVEF)为31%-40%的患者进行了一项回顾性队列研究,以评估空间QRS-T角与其他高级心电图(A-ECG)以及超声心动图元数据之间的关系,以及全因死亡率或用于二级预防的ICD植入情况。
通过超声心动图报告数据库识别出534例年龄≤75岁、LVEF为31%-40%的患者。对其中295例患者的数字12导联心电图进行回顾性匹配,然后为这些患者生成超声心动图和A-ECG元数据。应用数据挖掘来发现新的心电图和超声心动图风险标志物。使用机器学习开发一个模型来预测可能的结果。
49例患者(17%)发生了事件,定义为死亡(n = 16)或用于二级预防的ICD植入(n = 33)。在发生事件和未发生事件的患者中,72个参数(58个A-ECG参数、14个超声心动图参数)在单因素分析中存在差异(p<0.05)。在对多重性进行调整后,24个A-ECG参数和3个超声心动图参数仍存在差异(p<2×10-3)。这些参数包括从推导的心向量图水平面得出的后向与左向QRS环比率(先前与肺动脉压相关,p = 2×10-6);空间平均QRS-T角(134°对112°,p = 1.6×10-4);各种复极向量;以及先前描述的用于LVSD的5参数A-ECG评分(p = 4×10-6),该评分也与超声心动图整体纵向应变相关(R2 = - 0.51,P < 0.0001)。空间QRS-T角>110°对于二级ICD植入或全因死亡的调整后HR为3.4(95%CI 1.6至7.4),对于未来心力衰竭入院的调整后HR为4.1(95%CI 1.2至13.9)。随着疾病程度的增加,A-ECG和超声心动图变量之间的复杂性降低。
空间QRS-T角>110°与心律失常事件和全因死亡密切相关。对整体心电图和超声心动图元数据的深入分析揭示了潜在的关系,否则这些关系可能不会被发现。如果大规模应用,这些技术可能在未来的临床决策中证明是有用的。