Lajoie Isabelle, Tancredi Felipe B, Hoge Richard D
Département de physiologie moléculaire et intégrative, Institut de génie biomédical, Université de Montréal, Montreal, Quebec, Canada.
Department of Neurology and Neurosurgery, Montreal Neurological Institute, McGill University, Montreal, Quebec, Canada.
PLoS One. 2017 Mar 31;12(3):e0174932. doi: 10.1371/journal.pone.0174932. eCollection 2017.
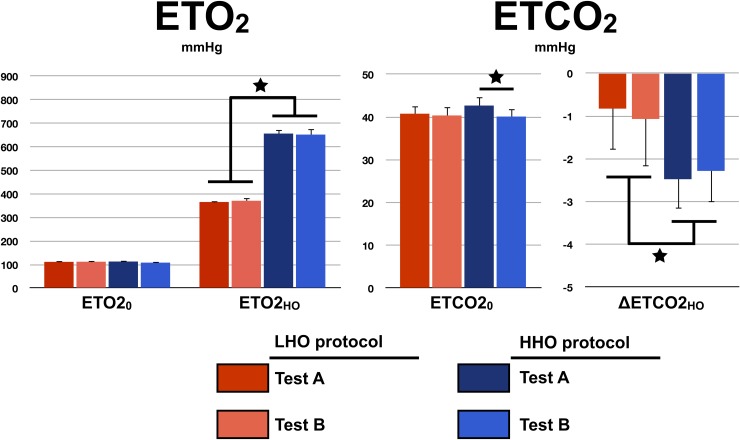
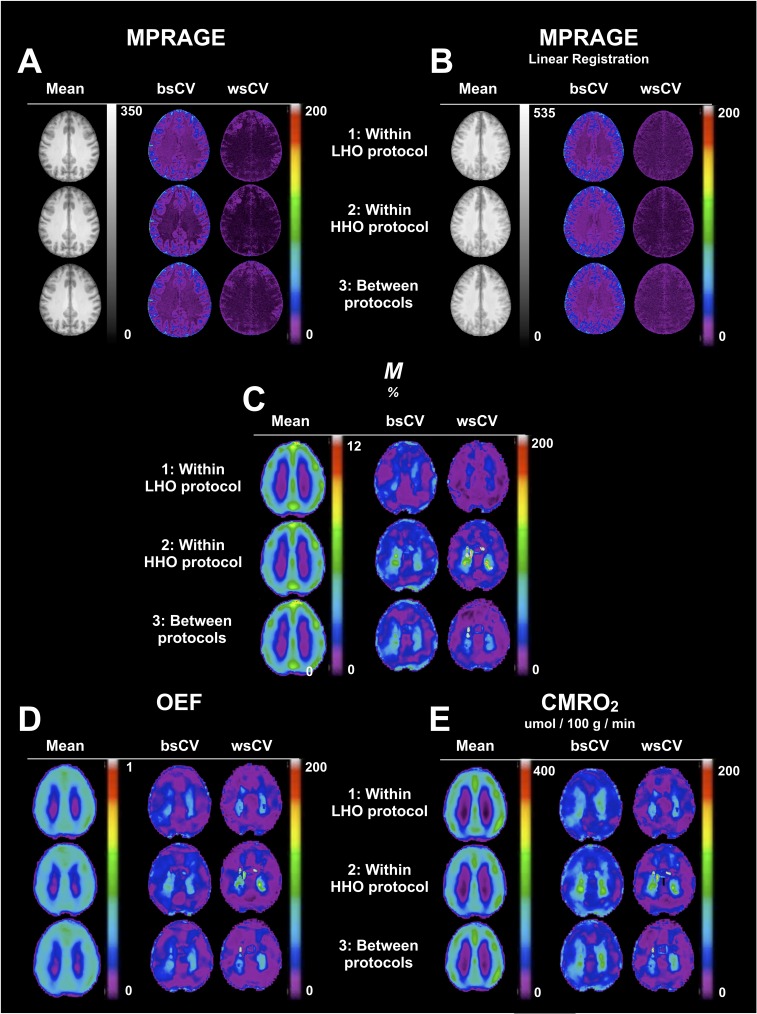
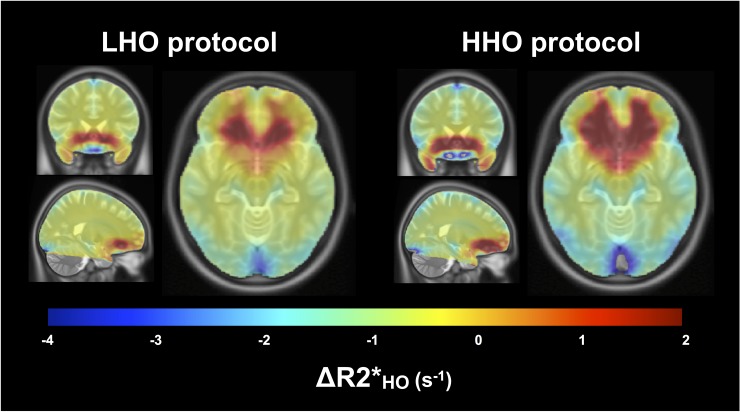
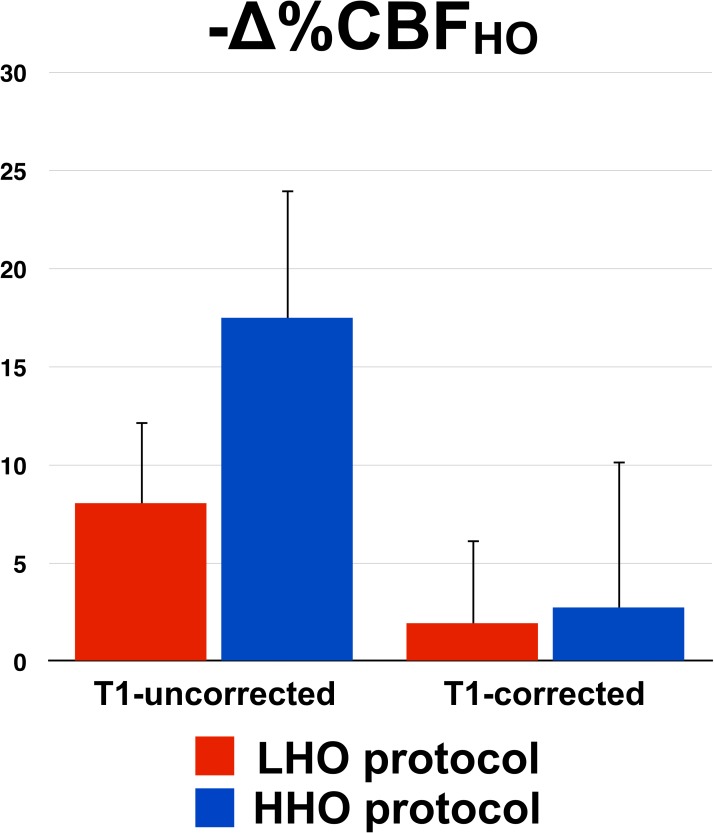
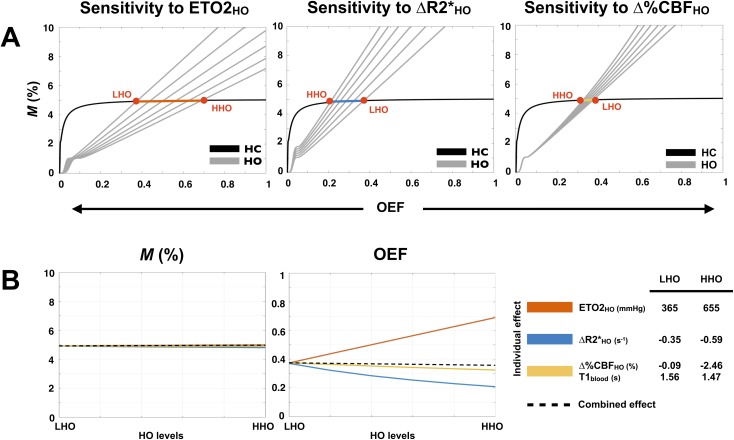
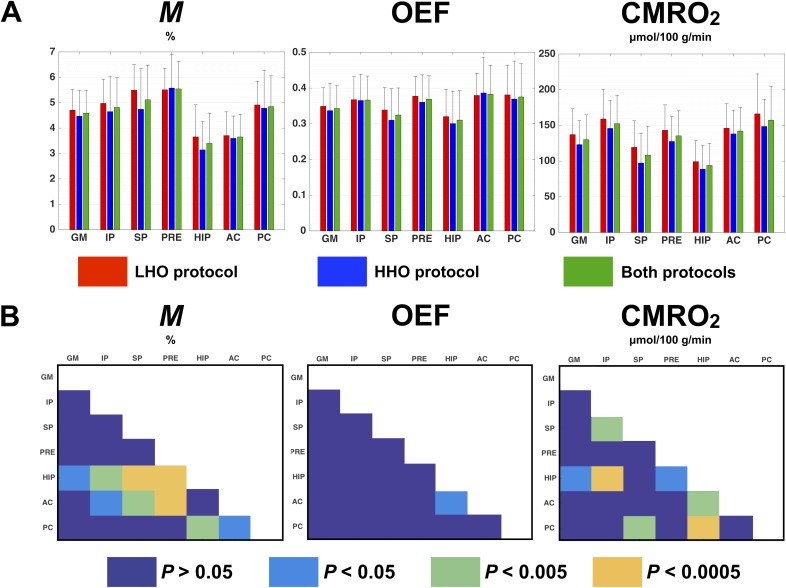
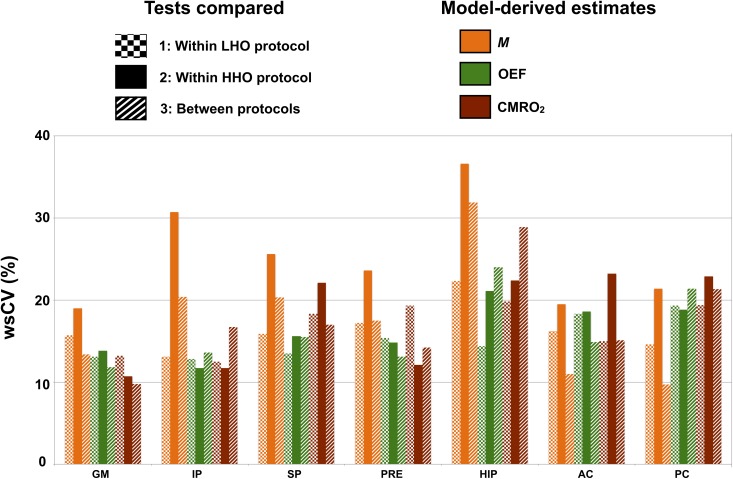
Recent calibrated fMRI techniques using combined hypercapnia and hyperoxia allow the mapping of resting cerebral metabolic rate of oxygen (CMRO2) in absolute units, oxygen extraction fraction (OEF) and calibration parameter M (maximum BOLD). The adoption of such technique necessitates knowledge about the precision and accuracy of the model-derived parameters. One of the factors that may impact the precision and accuracy is the level of oxygen provided during periods of hyperoxia (HO). A high level of oxygen may bring the BOLD responses closer to the maximum M value, and hence reduce the error associated with the M interpolation. However, an increased concentration of paramagnetic oxygen in the inhaled air may result in a larger susceptibility area around the frontal sinuses and nasal cavity. Additionally, a higher O2 level may generate a larger arterial blood T1 shortening, which require a bigger cerebral blood flow (CBF) T1 correction. To evaluate the impact of inspired oxygen levels on M, OEF and CMRO2 estimates, a cohort of six healthy adults underwent two different protocols: one where 60% of O2 was administered during HO (low HO or LHO) and one where 100% O2 was administered (high HO or HHO). The QUantitative O2 (QUO2) MRI approach was employed, where CBF and R2* are simultaneously acquired during periods of hypercapnia (HC) and hyperoxia, using a clinical 3 T scanner. Scan sessions were repeated to assess repeatability of results at the different O2 levels. Our T1 values during periods of hyperoxia were estimated based on an empirical ex-vivo relationship between T1 and the arterial partial pressure of O2. As expected, our T1 estimates revealed a larger T1 shortening in arterial blood when administering 100% O2 relative to 60% O2 (T1LHO = 1.56±0.01 sec vs. T1HHO = 1.47±0.01 sec, P < 4*10-13). In regard to the susceptibility artifacts, the patterns and number of affected voxels were comparable irrespective of the O2 concentration. Finally, the model-derived estimates were consistent regardless of the HO levels, indicating that the different effects are adequately accounted for within the model.
最近使用高碳酸血症和高氧联合的校准功能磁共振成像技术能够以绝对单位绘制静息脑氧代谢率(CMRO2)、氧摄取分数(OEF)和校准参数M(最大血氧水平依赖信号,BOLD)。采用这种技术需要了解模型衍生参数的精度和准确性。可能影响精度和准确性的因素之一是高氧(HO)期间提供的氧气水平。高氧水平可能会使BOLD反应更接近最大M值,从而减少与M插值相关的误差。然而,吸入空气中顺磁性氧浓度的增加可能会导致额窦和鼻腔周围更大的磁化率区域。此外,更高的氧气水平可能会产生更大的动脉血T1缩短,这需要更大的脑血流量(CBF)T1校正。为了评估吸入氧气水平对M、OEF和CMRO2估计值的影响,一组六名健康成年人接受了两种不同的方案:一种是在高氧期间给予60%的氧气(低高氧或LHO),另一种是给予100%的氧气(高高氧或HHO)。采用定量氧(QUO2)MRI方法,在高碳酸血症(HC)和高氧期间使用临床3T扫描仪同时采集CBF和R2*。重复扫描会话以评估不同氧气水平下结果的可重复性。我们在高氧期间的T1值是根据T1与动脉血氧分压之间的经验性体外关系估计的。正如预期的那样,我们的T1估计显示,相对于60%的氧气,给予100%的氧气时动脉血中的T1缩短更大(T1LHO = 1.56±0.01秒 vs. T1HHO = 1.47±0.01秒,P < 4×10-13)。关于磁化率伪影,无论氧气浓度如何,受影响体素的模式和数量都是可比的。最后,无论高氧水平如何,模型衍生的估计值都是一致的,这表明不同的影响在模型中得到了充分的考虑。