Morris Meghan D, Shiboski Stephen, Bruneau Julie, Hahn Judith A, Hellard Margaret, Prins Maria, Cox Andrea L, Dore Gregory, Grebely Jason, Kim Arthur Y, Lauer Georg M, Lloyd Andrew, Rice Thomas, Shoukry Naglaa, Maher Lisa, Page Kimberly
Department of Epidemiology and Biostatistics, University of California, San Francisco.
Centre Hospitalier de l'Universite de Montreal (CRCHUM), Université de Montréal, Quebec, Canada.
Clin Infect Dis. 2017 Apr 1;64(7):860-869. doi: 10.1093/cid/ciw869.
We determined temporal trends (1985-2011) in hepatitis C virus (HCV) incidence and associated behavioral exposures for people who inject drugs (PWID) from the United States (Boston, Baltimore, and San Francisco), Canada (Montreal), the Netherlands (Amsterdam), and Australia (Sydney and Melbourne).
Using population-based cohort data from HCV-negative PWID, we calculated overall and within-city HCV incidence trends, HCV rates by study enrollment period (1985-2011), and temporal trends in exposure behaviors. Poisson regression models estimated trends in HCV incidence over calendar-time. Survival models identified risk factors for HCV incidence across cities and estimated independent effects of city and calendar period on HCV infection risk.
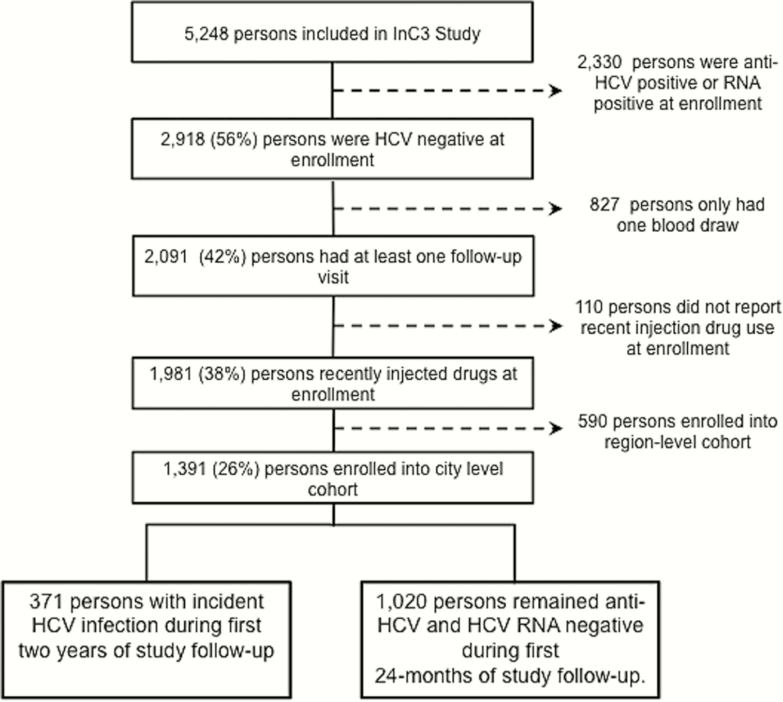
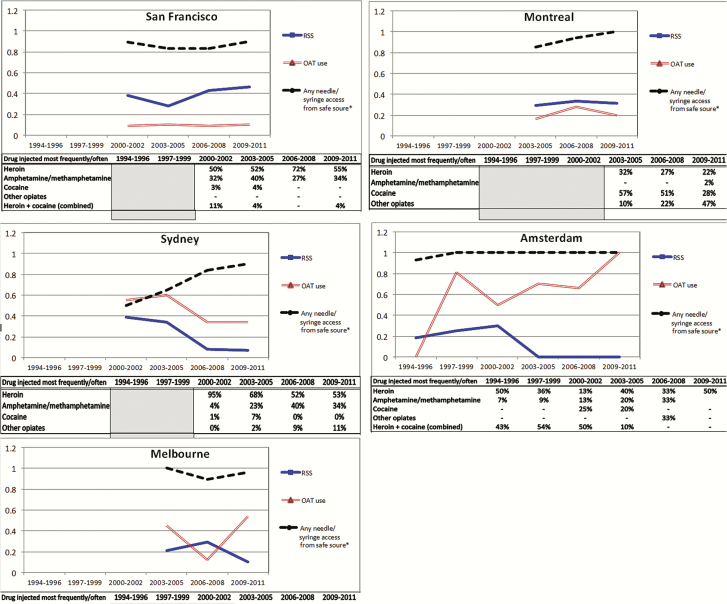
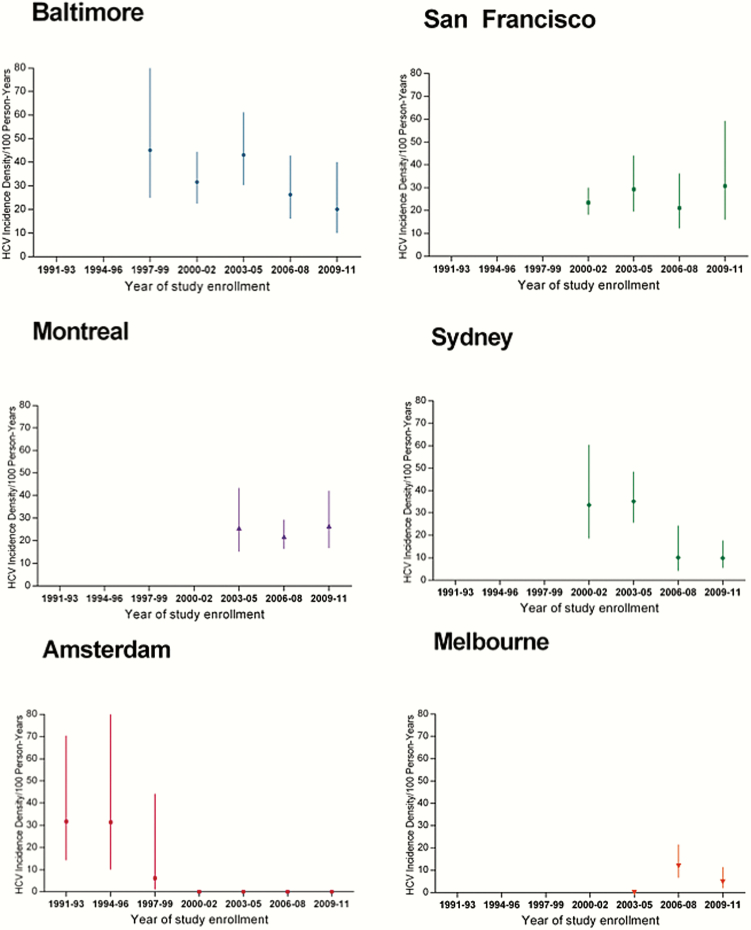
Among 1391 initially HCV-negative participants followed prospectively (1644.5 person-years of observation [PYO]), 371 HCV incident infections resulted in an overall incidence of 22.6 per 100 PYO (95% confidence interval [CI], 20.4-25.0). Incidence was highest and remained elevated in Baltimore (32.6/100 PYO), San Francisco (24.7/100 PYO), and Montreal (23.5/100 PYO), lowest in Melbourne and Amsterdam (7.5/100 PYO and 13.1/100 PYO, respectively), and moderate (21.4/100 PYO) in Sydney. Higher rates of syringe and equipment sharing and lower prevalence of opioid agonist therapy were associated with HCV incidence in cities with the highest incidence. Risk for infection dropped by 18% for every 3-year increase in calendar-time (adjusted hazard ratio, 0.8 [95% CI, .8-.9]) in the multivariable model.
Differences in prevention strategies and injecting contexts may explain the ongoing high HCV incidence in these North American cities and emphasize the need for scale-up of opioid agonist therapy and increased coverage of needle and syringe programs in North America.
我们确定了来自美国(波士顿、巴尔的摩和旧金山)、加拿大(蒙特利尔)、荷兰(阿姆斯特丹)和澳大利亚(悉尼和墨尔本)的注射吸毒者(PWID)中丙型肝炎病毒(HCV)发病率及相关行为暴露的时间趋势(1985 - 2011年)。
利用来自HCV阴性PWID的基于人群的队列数据,我们计算了总体及城市内的HCV发病率趋势、按研究入组时间(1985 - 2011年)划分的HCV发病率以及暴露行为的时间趋势。泊松回归模型估计了日历时间内HCV发病率的趋势。生存模型确定了各城市HCV发病的危险因素,并估计了城市和日历时期对HCV感染风险的独立影响。
在1391名最初HCV阴性且接受前瞻性随访的参与者中(1644.5人年观察期[PYO]),371例HCV新发感染导致总体发病率为每100 PYO 22.6例(95%置信区间[CI],20.4 - 25.0)。发病率在巴尔的摩(32.6/100 PYO)、旧金山(24.7/100 PYO)和蒙特利尔(23.5/100 PYO)最高且持续升高,在墨尔本和阿姆斯特丹最低(分别为7.5/100 PYO和13.1/100 PYO),在悉尼为中等水平(2,1.4/100 PYO)。在发病率最高的城市,更高的注射器和设备共用率以及更低的阿片类激动剂治疗普及率与HCV发病相关。在多变量模型中,日历时间每增加3年,感染风险下降18%(调整后风险比,0.8 [95% CI,0.8 - 0.9])。
预防策略和注射环境的差异可能解释了这些北美城市持续的高HCV发病率,并强调了在北美扩大阿片类激动剂治疗规模以及增加针头和注射器项目覆盖范围的必要性。