School of Medicine and Health Sciences, Monash University, Bandar Sunway, Malaysia
Accident and Emergency Directorate, Komfo Anokye Teaching Hospital, Kumasi, Ghana.
J Am Heart Assoc. 2017 Apr 1;6(4):e004706. doi: 10.1161/JAHA.116.004706.
Randomized control trials of statins have not demonstrated significant benefits in outcomes of heart failure (HF). However, randomized control trials may not always be generalizable. The aim was to determine whether statin and statin type-lipophilic or -hydrophilic improve long-term outcomes in Africans with HF.
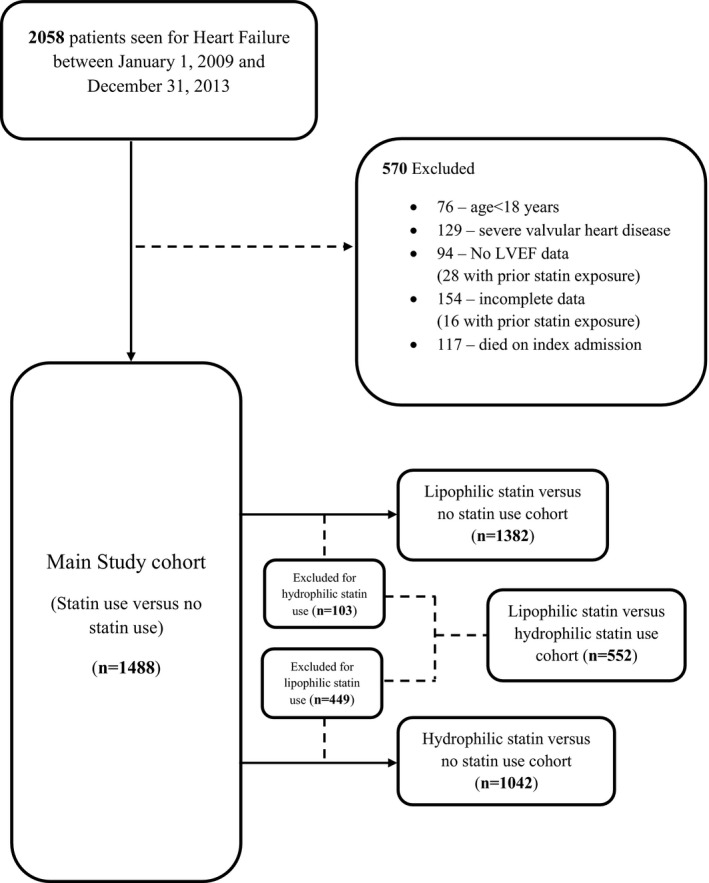
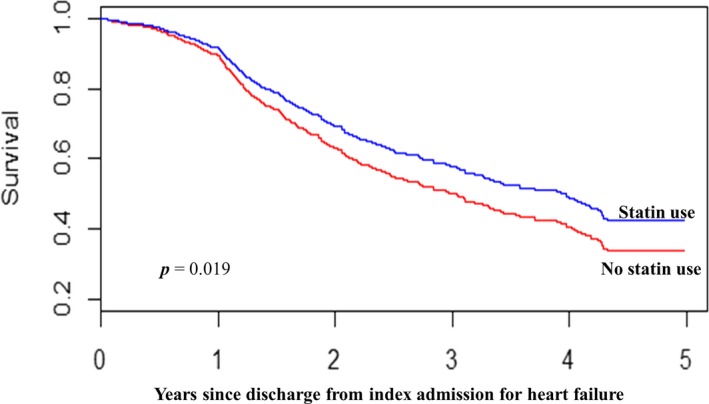
This was a retrospective longitudinal study of HF patients aged ≥18 years hospitalized at a tertiary healthcare center between January 1, 2009 and December 31, 2013 in Ghana. Patients were eligible if they were discharged from first admission for HF (index admission) and followed up to time of all-cause, cardiovascular, and HF mortality or end of study. Multivariable time-dependent Cox model and inverse-probability-of-treatment weighting of marginal structural model were used to estimate associations between statin treatment and outcomes. Adjusted hazard ratios were also estimated for lipophilic and hydrophilic statin compared with no statin use. The study included 1488 patients (mean age 60.3±14.2 years) with 9306 person-years of observation. Using the time-dependent Cox model, the 5-year adjusted hazard ratios with 95% CI for statin treatment on all-cause, cardiovascular, and HF mortality were 0.68 (0.55-0.83), 0.67 (0.54-0.82), and 0.63 (0.51-0.79), respectively. Use of inverse-probability-of-treatment weighting resulted in estimates of 0.79 (0.65-0.96), 0.77 (0.63-0.96), and 0.77 (0.61-0.95) for statin treatment on all-cause, cardiovascular, and HF mortality, respectively, compared with no statin use.
Among Africans with HF, statin treatment was associated with significant reduction in mortality.
他汀类药物的随机对照试验并未显示出对心力衰竭(HF)结局的显著益处。然而,随机对照试验并不总是具有普遍性。本研究旨在确定在非洲 HF 患者中,他汀类药物及其亲脂性或亲水性是否能改善长期结局。
这是一项回顾性纵向研究,纳入了 2009 年 1 月 1 日至 2013 年 12 月 31 日期间在加纳一家三级保健中心住院的年龄≥18 岁的 HF 患者。如果患者符合以下标准,即可入选:从首次 HF 入院(索引入院)出院,并随访至全因、心血管和 HF 死亡或研究结束。使用多变量时间依赖性 Cox 模型和边际结构模型的逆概率治疗加权来估计他汀类药物治疗与结局之间的关联。还估计了与未使用他汀类药物相比,亲脂性和亲水性他汀类药物的调整后危险比。该研究纳入了 1488 例患者(平均年龄 60.3±14.2 岁),观察了 9306 人年。使用时间依赖性 Cox 模型,他汀类药物治疗的 5 年调整后的全因、心血管和 HF 死亡的危险比及其 95%可信区间分别为 0.68(0.55-0.83)、0.67(0.54-0.82)和 0.63(0.51-0.79)。使用逆概率治疗加权的结果估计为,与未使用他汀类药物相比,他汀类药物治疗的全因、心血管和 HF 死亡的危险比分别为 0.79(0.65-0.96)、0.77(0.63-0.96)和 0.77(0.61-0.95)。
在非洲 HF 患者中,他汀类药物治疗与死亡率显著降低相关。