van Nieuwkoop Cees, van der Starre Willize E, Stalenhoef Janneke E, van Aartrijk Anna M, van der Reijden Tanny J K, Vollaard Albert M, Delfos Nathalie M, van 't Wout Jan W, Blom Jeanet W, Spelt Ida C, Leyten Eliane M S, Koster Ted, Ablij Hans C, van der Beek Martha T, Knol Mirjam J, van Dissel Jaap T
Department of Internal Medicine, Haga Teaching Hospital, Els-Borst Eilersplein 245, 2545 AA, The Hague, The Netherlands.
Department of Infectious Diseases, Leiden University Medical Center, Leiden, The Netherlands.
BMC Med. 2017 Apr 3;15(1):70. doi: 10.1186/s12916-017-0835-3.
In adults with febrile urinary tract infection (fUTI), data on optimal treatment duration in patients other than non-pregnant women without comorbidities are lacking.
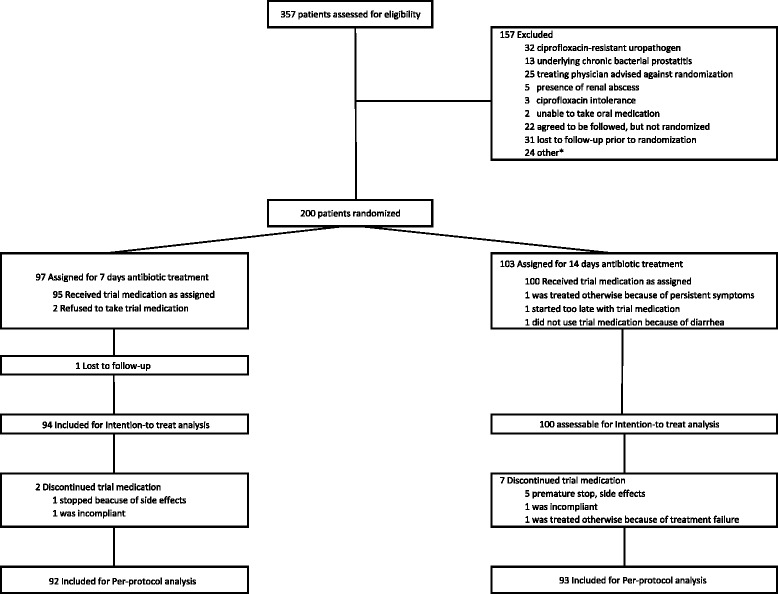
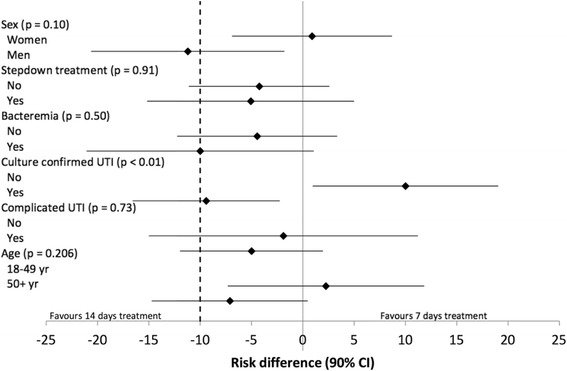
A randomized placebo-controlled, double-blind, non-inferiority trial among 35 primary care centers and 7 emergency departments of regional hospitals in the Netherlands. Women and men aged ≥ 18 years with a diagnosis of fUTI were randomly assigned to receive antibiotic treatment for 7 or 14 days (the second week being ciprofloxacin 500 mg or placebo orally twice daily). Patients indicated to receive antimicrobial treatment for at least 14 days were excluded from randomization. The primary endpoint was the clinical cure rate through the 10- to 18-day post-treatment visit with preset subgroup analysis including sex. Secondary endpoints were bacteriologic cure rate at 10-18 days post-treatment and clinical cure at 70-84 days post-treatment.
Of 357 patients included, 200 were eligible for randomization; 97 patients were randomly assigned to 7 days and 103 patients to 14 days of treatment. Overall, short-term clinical cure occurred in 85 (90%) patients treated for 7 days and in 94 (95%) of those treated for 14 days (difference -4.5%; 90% CI, -10.7 to 1.7; P = 0.072, non-inferiority not confirmed). In women, clinical cure was 94% and 93% in those treated for 7 and 14 days, respectively (difference 0.9; 90% CI, -6.9 to 8.7, P = 0.011, non-inferiority confirmed) and, in men, this was 86% versus 98% (difference -11.2; 90% CI -20.6 to -1.8, P = 0.025, inferiority confirmed). The bacteriologic cure rate was 93% versus 97% (difference -4.3%; 90% CI, -9.7 to 1.2, P = 0.041) and the long-term clinical cure rate was 92% versus 91% (difference 1.6%; 90% CI, -5.3 to 8.4; P = 0.005) for 7 days versus 14 days of treatment, respectively. In the subgroups of men and women, long-term clinical cure rates met the criteria for non-inferiority, indicating there was no difference in the need for antibiotic retreatment for UTI during 70-84 days follow-up post-treatment.
Women with fUTI can be treated successfully with antibiotics for 7 days. In men, 7 days of antibiotic treatment for fUTI is inferior to 14 days during short-term follow-up but it is non-inferior when looking at longer follow-up.
The study was registered at ClinicalTrials.gov [ NCT00809913 ; December 16, 2008] and trialregister.nl [ NTR1583 ; December 19, 2008].
在患有发热性尿路感染(fUTI)的成年人中,除无合并症的非妊娠女性外,其他患者最佳治疗疗程的数据尚缺。
在荷兰的35个初级保健中心和7个地区医院急诊科进行一项随机、安慰剂对照、双盲、非劣效性试验。年龄≥18岁且诊断为fUTI的女性和男性被随机分配接受7天或14天的抗生素治疗(第二周口服环丙沙星500mg或安慰剂,每日两次)。被指定接受至少14天抗菌治疗的患者被排除在随机分组之外。主要终点是治疗后10至18天的临床治愈率,并进行预设的包括性别的亚组分析。次要终点是治疗后10 - 18天的细菌学治愈率和治疗后70 - 84天的临床治愈率。
在纳入的357例患者中,200例符合随机分组条件;97例患者被随机分配接受7天治疗,103例患者接受14天治疗。总体而言,接受7天治疗的85例(90%)患者和接受14天治疗的94例(95%)患者实现了短期临床治愈(差异 -4.5%;90%CI,-10.7至1.7;P = 0.072,未证实非劣效性)。在女性中,接受7天和14天治疗的患者临床治愈率分别为94%和93%(差异0.9;90%CI,-6.9至8.7,P = 0.011,证实非劣效性),在男性中,分别为86%和98%(差异 -11.2;90%CI -20.6至 -1.8,P = 0.025,证实劣效性)。治疗7天和14天的细菌学治愈率分别为93%和97%(差异 -4.3%;90%CI,-9.7至1.2,P = 0.041),长期临床治愈率分别为92%和91%(差异1.6%;90%CI,-5.3至8.4;P = 0.005)。在男性和女性亚组中,长期临床治愈率符合非劣效性标准,表明治疗后70 - 84天随访期间尿路感染抗生素再治疗需求无差异。
患有fUTI的女性使用抗生素治疗7天可成功治愈。在男性中,fUTI的7天抗生素治疗在短期随访中劣于14天,但在较长随访期时非劣效。
该研究在ClinicalTrials.gov [NCT00809913;2008年12月16日]和trialregister.nl [NTR1583;2008年12月19日]注册。