White River Junction VA Medical Center, White River Junction, VT, USA; Section of Urology and Norris Cotton Cancer Center, Dartmouth Hitchcock Medical Center, Lebanon, NH, USA; The Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine at Dartmouth College, Lebanon, NH, USA.
Department of Urology, University of Pittsburgh, Pittsburgh, PA, USA; Center for Research on Health Care, Division of General Internal Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
Eur Urol. 2017 Nov;72(5):712-735. doi: 10.1016/j.eururo.2017.03.028. Epub 2017 Mar 31.
Some of the high costs of robot-assisted radical prostatectomy (RARP), intensity-modulated radiotherapy (IMRT), and proton beam therapy may be offset by better outcomes or less resource use during the treatment episode.
To systematically review the literature to identify the key economic trade-offs implicit in a particular treatment choice for prostate cancer.
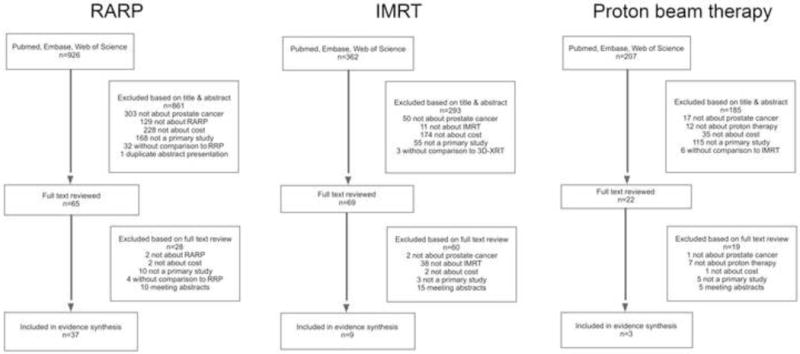
We systematically reviewed the literature according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement and protocol. We searched Medline, Embase, and Web of Science for articles published between January 2001 and July 2016, which compared the treatment costs of RARP, IMRT, or proton beam therapy to the standard treatment. We identified 37, nine, and three studies, respectively.
RARP is costlier than radical retropubic prostatectomy for hospitals and payers. However, RARP has the potential for a moderate cost advantage for payers and society over a longer time horizon when optimal cancer and quality-of-life outcomes are achieved. IMRT is more expensive from a payer's perspective compared with three-dimensional conformal radiotherapy, but also more cost effective when defined by an incremental cost effectiveness ratio <$50 000 per quality-adjusted life year. Proton beam therapy is costlier than IMRT and its cost effectiveness remains unclear given the limited comparative data on outcomes. Using the Grades of Recommendation, Assessment, Development and Evaluation approach, the quality of evidence was low for RARP and IMRT, and very low for proton beam therapy.
Treatment with new versus traditional technologies is costlier. However, given the low quality of evidence and the inconsistencies across studies, the precise difference in costs remains unclear. Attempts to estimate whether this increased cost is worth the expense are hampered by the uncertainty surrounding improvements in outcomes, such as cancer control and side effects of treatment. If the new technologies can consistently achieve better outcomes, then they may be cost effective.
We review the cost and cost effectiveness of robot-assisted radical prostatectomy, intensity-modulated radiotherapy, and proton beam therapy in prostate cancer treatment. These technologies are costlier than their traditional counterparts. It remains unclear whether their use is associated with improved cure and reduced morbidity, and whether the increased cost is worth the expense.
机器人辅助根治性前列腺切除术(RARP)、调强放疗(IMRT)和质子束治疗的一些高昂费用可能会因治疗过程中更好的结果或更少的资源利用而得到弥补。
系统地回顾文献,以确定前列腺癌特定治疗方案中隐含的关键经济权衡。
我们根据系统评价和荟萃分析的首选报告项目(PRISMA)声明和方案,系统地回顾了文献。我们在 Medline、Embase 和 Web of Science 中搜索了 2001 年 1 月至 2016 年 7 月期间发表的比较 RARP、IMRT 或质子束治疗与标准治疗的治疗费用的文章。我们分别确定了 37、9 和 3 项研究。
RARP 比根治性前列腺切除术对医院和支付者来说成本更高。然而,在更长的时间范围内,当获得最佳的癌症和生活质量结果时,RARP 对支付者和社会具有适度的成本优势。从支付者的角度来看,与三维适形放疗相比,IMRT 更昂贵,但当定义为增量成本效益比<50000 美元/质量调整生命年时,也更具成本效益。质子束治疗比 IMRT 更昂贵,但其成本效益仍不清楚,因为关于结果的比较数据有限。使用推荐、评估、开发和评估方法的等级,RARP 和 IMRT 的证据质量低,质子束治疗的证据质量非常低。
新的治疗技术比传统技术更昂贵。然而,鉴于证据质量低以及研究之间的不一致性,确切的成本差异仍不清楚。如果新的技术能够始终如一地获得更好的结果,那么它们可能具有成本效益。
我们回顾了机器人辅助根治性前列腺切除术、调强放疗和质子束治疗在前列腺癌治疗中的成本和成本效益。这些技术比传统技术更昂贵。目前尚不清楚它们的使用是否与改善疗效和降低治疗副作用相关,以及增加的成本是否值得。