1Department of Population Health,London School of Hygiene & Tropical Medicine,London WC1E 7HT,UK.
3Public Health Foundation of India, Delhi NCR,Institutional Area Gurgaon,India.
Public Health Nutr. 2017 Aug;20(11):1963-1972. doi: 10.1017/S1368980017000416. Epub 2017 Apr 3.
Undernutrition and non-communicable disease (NCD) are important public health issues in India, yet their relationship with dietary patterns is poorly understood. The current study identified distinct dietary patterns and their association with micronutrient undernutrition (Ca, Fe, Zn) and NCD risk factors (underweight, obesity, waist:hip ratio, hypertension, total:HDL cholesterol, diabetes).
Data were from the cross-sectional Indian Migration Study, including semi-quantitative FFQ. Distinct dietary patterns were identified using finite mixture modelling; associations with NCD risk factors were assessed using mixed-effects logistic regression models.
India.
Migrant factory workers, their rural-dwelling siblings and urban non-migrants. Participants (7067 adults) resided mainly in Karnataka, Andhra Pradesh, Maharashtra and Uttar Pradesh.
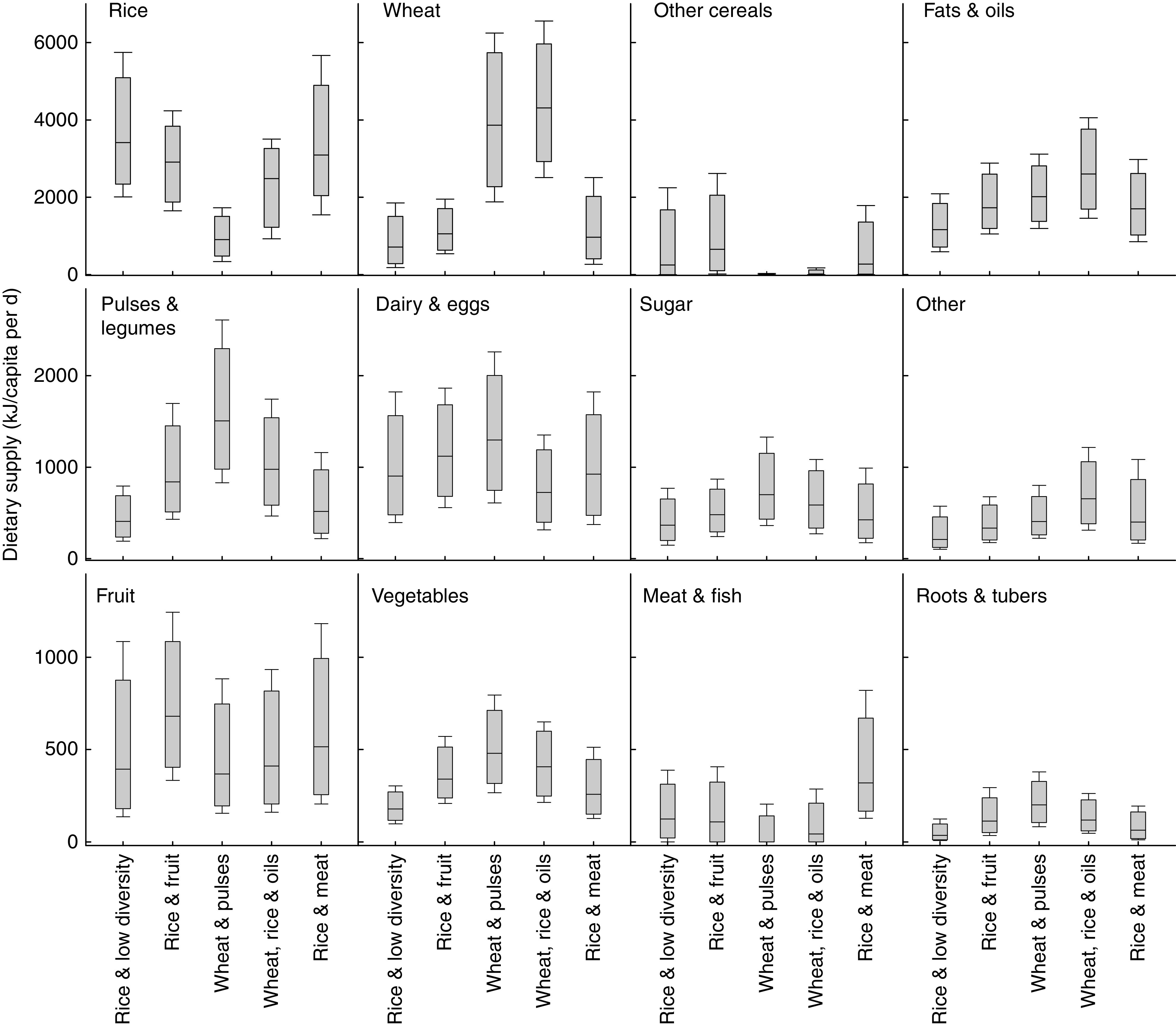
Five distinct, regionally distributed, dietary patterns were identified, with rice-based patterns in the south and wheat-based patterns in the north-west. A rice-based pattern characterised by low energy consumption and dietary diversity ('Rice & low diversity') was consumed predominantly by adults with little formal education in rural settings, while a rice-based pattern with high fruit consumption ('Rice & fruit') was consumed by more educated adults in urban settings. Dietary patterns met WHO macronutrient recommendations, but some had low micronutrient contents. Dietary pattern membership was associated with several NCD risk factors.
Five distinct dietary patterns were identified, supporting sub-national assessments of the implications of dietary patterns for various health, food system or environment outcomes.
在印度,营养不良和非传染性疾病(NCD)是重要的公共卫生问题,但人们对它们与饮食模式的关系知之甚少。本研究旨在确定不同的饮食模式及其与微量营养素营养不良(Ca、Fe、Zn)和 NCD 风险因素(体重不足、肥胖、腰臀比、高血压、总胆固醇/高密度脂蛋白胆固醇、糖尿病)的关系。
数据来自横断面印度移民研究,包括半定量食物频率问卷。采用有限混合模型识别不同的饮食模式;采用混合效应逻辑回归模型评估与 NCD 风险因素的关联。
印度。
工厂移民工人及其农村居住的兄弟姐妹和城市非移民。参与者(7067 名成年人)主要居住在卡纳塔克邦、安得拉邦、马哈拉施特拉邦和北方邦。
确定了 5 种不同的、分布在不同地区的饮食模式,南部以米饭为基础,西北部以小麦为基础。以低能量摄入和饮食多样性为特征的以米饭为基础的模式(“米饭和低多样性”)主要由农村地区受教育程度较低的成年人消费,而以高水果消费为特征的以米饭为基础的模式(“米饭和水果”)则由城市地区受教育程度较高的成年人消费。饮食模式符合世卫组织的宏量营养素建议,但某些模式的微量营养素含量较低。饮食模式的组成与多种 NCD 风险因素相关。
确定了 5 种不同的饮食模式,支持对饮食模式对各种健康、食品系统或环境结果的影响进行国家以下层面的评估。