Yannas Ioannis V, Tzeranis Dimitrios S, So Peter T C
Department of Mechanical Engineering, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Department of Biological Engineering, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Wound Repair Regen. 2017 Apr;25(2):177-191. doi: 10.1111/wrr.12516. Epub 2017 Apr 27.
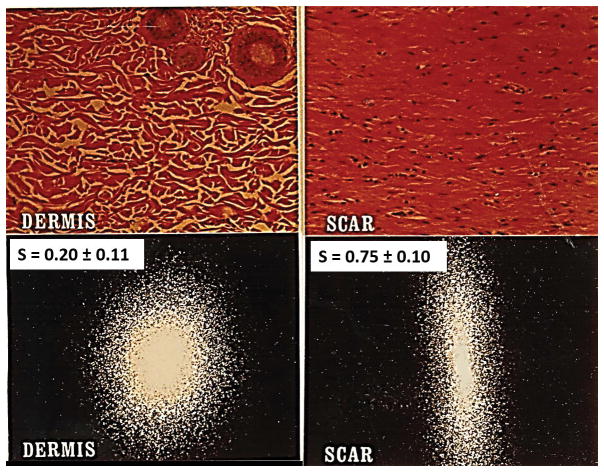
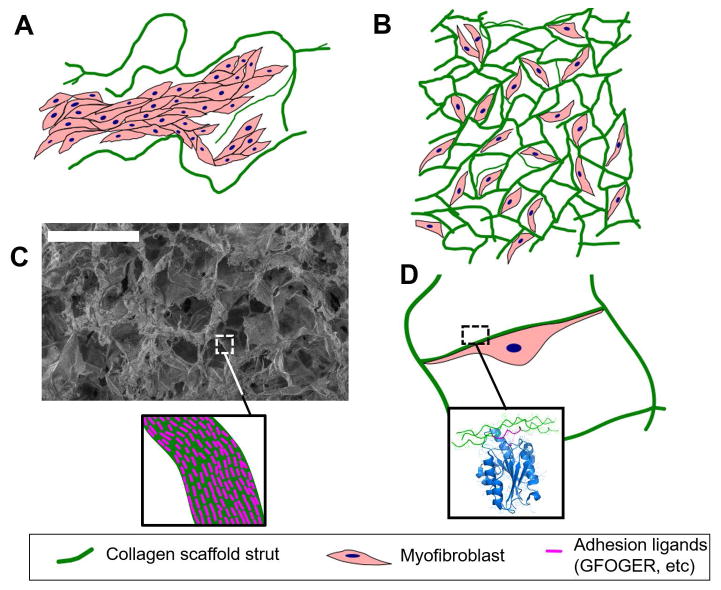
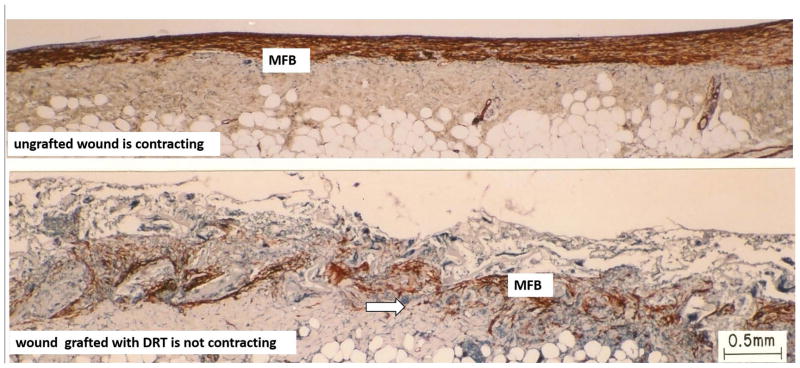
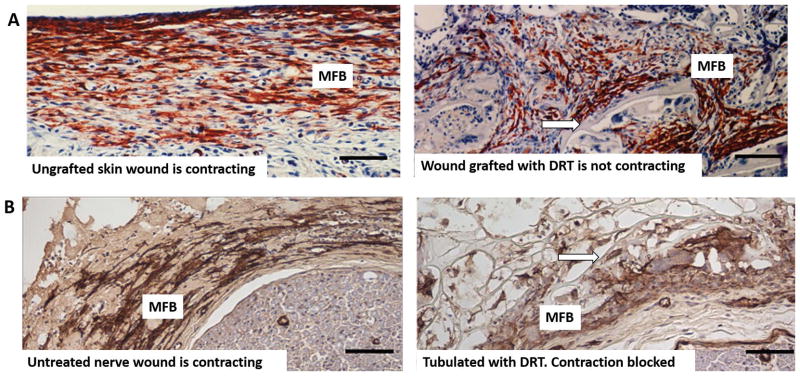
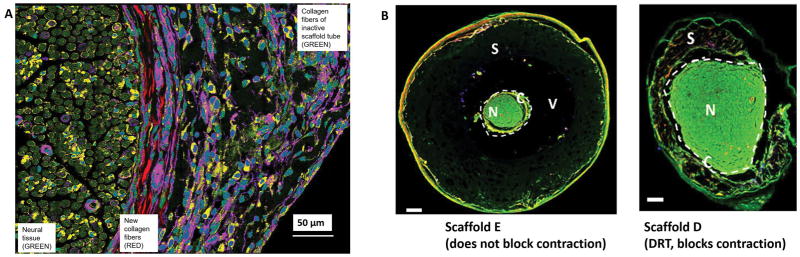
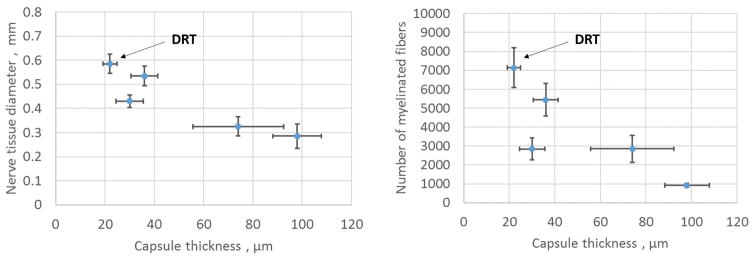
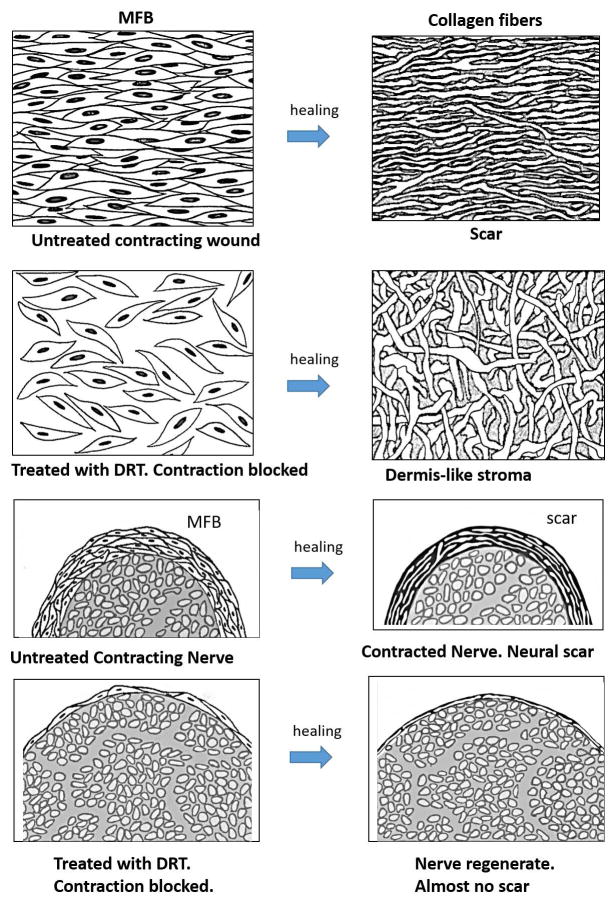
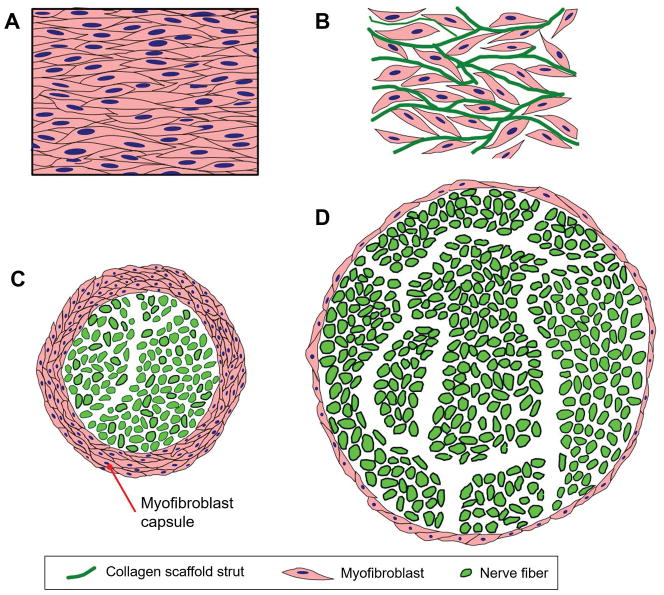
We review the mounting evidence that regeneration is induced in wounds in skin and peripheral nerves by a simple modification of the wound healing process. Here, the process of induced regeneration is compared to the other two well-known processes by which wounds close, i.e., contraction and scar formation. Direct evidence supports the hypothesis that the mechanical force of contraction (planar in skin wounds, circumferential in nerve wounds) is the driver guiding the orientation of assemblies of myofibroblasts (MFB) and collagen fibers during scar formation in untreated wounds. We conclude that scar formation depends critically on wound contraction and is, therefore, a healing process secondary to contraction. Wound contraction and regeneration did not coincide during healing in a number of experimental models of spontaneous (untreated) regeneration described in the literature. Furthermore, in other studies in which an efficient contraction-blocker, a collagen scaffold named dermis regeneration template (DRT), and variants of it, were grafted on skin wounds or peripheral nerve wounds, regeneration was systematically observed in the absence of contraction. We conclude that contraction and regeneration are mutually antagonistic processes. A dramatic change in the phenotype of MFB was observed when the contraction-blocking scaffold DRT was used to treat wounds in skin and peripheral nerves. The phenotype change was directly observed as drastic reduction in MFB density, dispersion of MFB assemblies and loss of alignment of the long MFB axes. These observations were explained by the evidence of a surface-biological interaction of MFB with the scaffold, specifically involving binding of MFB integrins α β and α β to ligands GFOGER and GLOGER naturally present on the surface of the collagen scaffold. In summary, we show that regeneration of wounded skin and peripheral nerves in the adult mammal can be induced simply by appropriate control of wound contraction, rather than of scar formation.
我们回顾了越来越多的证据,即通过对伤口愈合过程进行简单的调整,可以在皮肤和周围神经的伤口中诱导再生。在此,将诱导再生过程与伤口闭合的其他两个众所周知的过程,即收缩和瘢痕形成进行比较。直接证据支持这样的假说:在未处理伤口形成瘢痕的过程中,收缩的机械力(皮肤伤口中为平面力,神经伤口中为圆周力)是引导肌成纤维细胞(MFB)和胶原纤维组装方向的驱动力。我们得出结论,瘢痕形成严重依赖于伤口收缩,因此是继收缩之后的愈合过程。在文献中描述的许多自发(未处理)再生的实验模型中,伤口收缩和再生在愈合过程中并不一致。此外,在其他研究中,将一种有效的收缩阻滞剂、一种名为真皮再生模板(DRT)的胶原支架及其变体移植到皮肤伤口或周围神经伤口上,在没有收缩的情况下系统地观察到了再生。我们得出结论,收缩和再生是相互拮抗的过程。当使用收缩阻断支架DRT治疗皮肤和周围神经的伤口时,观察到MFB的表型发生了显著变化。直接观察到表型变化表现为MFB密度急剧降低、MFB组装分散以及长MFB轴排列丧失。这些观察结果可以通过MFB与支架的表面生物相互作用的证据来解释,具体涉及MFB整合素αβ和αβ与胶原支架表面天然存在的配体GFOGER和GLOGER的结合。总之,我们表明,成年哺乳动物受伤皮肤和周围神经的再生可以通过适当控制伤口收缩而不是瘢痕形成来简单地诱导。