The National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care West (NIHR CLAHRC West) at University Hospitals Bristol NHS Foundation Trust, Bristol, UK.
School of Social and Community Medicine, University of Bristol, Bristol, UK.
BMJ Open. 2017 Apr 7;7(4):e012674. doi: 10.1136/bmjopen-2016-012674.
To summarise evidence on temporary discontinuation of medications to prevent acute kidney injury (AKI).
Systematic review and meta-analysis of randomised and non-randomised studies.
Adults taking diuretics, ACE inhibitors (ACEI), angiotensin receptor blockers (ARB), direct renin inhibitors, non-steroidal anti-inflammatories, metformin or sulfonylureas, experiencing intercurrent illnesses, radiological or surgical procedures.
Temporary discontinuation of any of the medications of interest.
Risk of AKI. Secondary outcome measures were estimated glomerular filtration rate and creatinine post-AKI, urea, systolic and diastolic blood pressure, death, clinical outcomes and biomarkers.
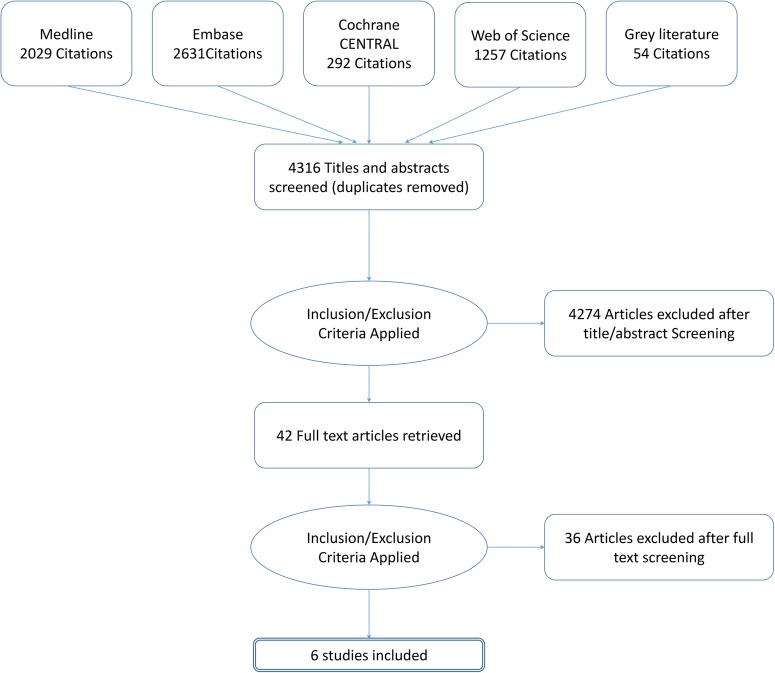
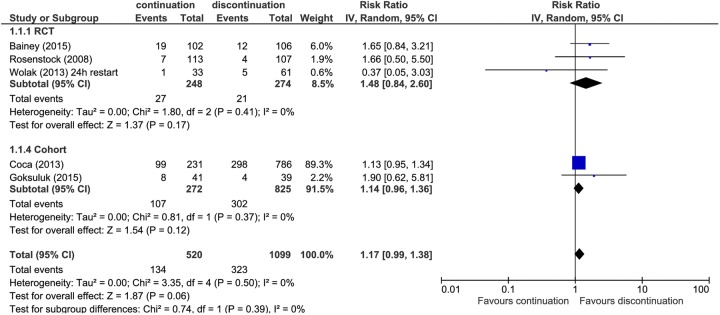
6 studies were included (1663 participants), 3 randomised controlled trials (RCTs) and 3 prospective cohort studies. The mean age ranged from 65 to 73 years, and the proportion of women ranged from 31% to 52%. All studies were in hospital settings; 5 evaluated discontinuation of medication prior to coronary angiography and 1 prior to cardiac surgery. 5 studies evaluated discontinuation of ACEI and ARBs and 1 small cohort study looked at discontinuation of non-steroidal anti-inflammatory drugs. No studies evaluated discontinuation of medication in the community following an acute intercurrent illness. There was an increased risk of AKI of around 15% in those in whom medication was continued compared with those in whom it was discontinued (relative risk (RR) 1.17, 95% CI 0.99 to 1.38; 5 studies). When only results from RCTs were pooled, the increase in risk was almost 50% (RR 1.48, 95% CI 0.84 to 2.60; 3 RCTs), but the CI was wider. There was no difference between groups for any secondary outcomes.
There is low-quality evidence that withdrawal of ACEI/ARBs prior to coronary angiography and cardiac surgery may reduce the incidence of AKI. There is no evidence of the impact of drug cessation interventions on AKI incidence during intercurrent illness in primary or secondary care.
PROSPERO CRD42015023210.
总结预防急性肾损伤(AKI)的药物临时停药的证据。
随机和非随机研究的系统评价和荟萃分析。
服用利尿剂、血管紧张素转换酶抑制剂(ACEI)、血管紧张素受体阻滞剂(ARB)、直接肾素抑制剂、非甾体抗炎药、二甲双胍或磺酰脲类药物的成年人,患有急性病、影像学或手术。
任何有兴趣的药物临时停药。
AKI 风险。次要结局指标为 AKI 后估计肾小球滤过率和肌酐、尿素、收缩压和舒张压、死亡率、临床结局和生物标志物。
纳入 6 项研究(1663 名参与者),包括 3 项随机对照试验(RCT)和 3 项前瞻性队列研究。平均年龄范围为 65 至 73 岁,女性比例范围为 31%至 52%。所有研究均在医院环境中进行;5 项评估了在冠状动脉造影前停药,1 项评估了在心脏手术后停药。5 项研究评估了 ACEI 和 ARB 的停药,1 项小队列研究评估了非甾体抗炎药的停药。没有研究评估在急性急性病后在社区中停止药物治疗的情况。与继续用药相比,停药的患者 AKI 风险增加约 15%(相对风险(RR)1.17,95%CI 0.99 至 1.38;5 项研究)。当仅汇总 RCT 的结果时,风险增加近 50%(RR 1.48,95%CI 0.84 至 2.60;3 项 RCT),但 CI 更宽。两组之间的任何次要结局均无差异。
低质量证据表明,在冠状动脉造影和心脏手术后停用 ACEI/ARB 可能会降低 AKI 的发生率。在初级或二级保健中,没有证据表明药物停药干预对急性病期间 AKI 发生率的影响。
PROSPERO CRD42015023210。