de Ruiter Quirina M, Gijsberts Crystel M, Hazenberg Constantijn E, Moll Frans L, van Herwaarden Joost A
1 Department of Vascular Surgery, University Medical Center Utrecht, the Netherlands.
2 ICIN-Netherlands Heart Institute, Utrecht, the Netherlands.
J Endovasc Ther. 2017 Jun;24(3):425-434. doi: 10.1177/1526602817697188. Epub 2017 Apr 10.
To determine which patient and C-arm characteristics are the strongest predictors of intraoperative patient radiation dose rates (DRs) during endovascular aneurysm repair (EVAR) procedures and create a patient risk chart.
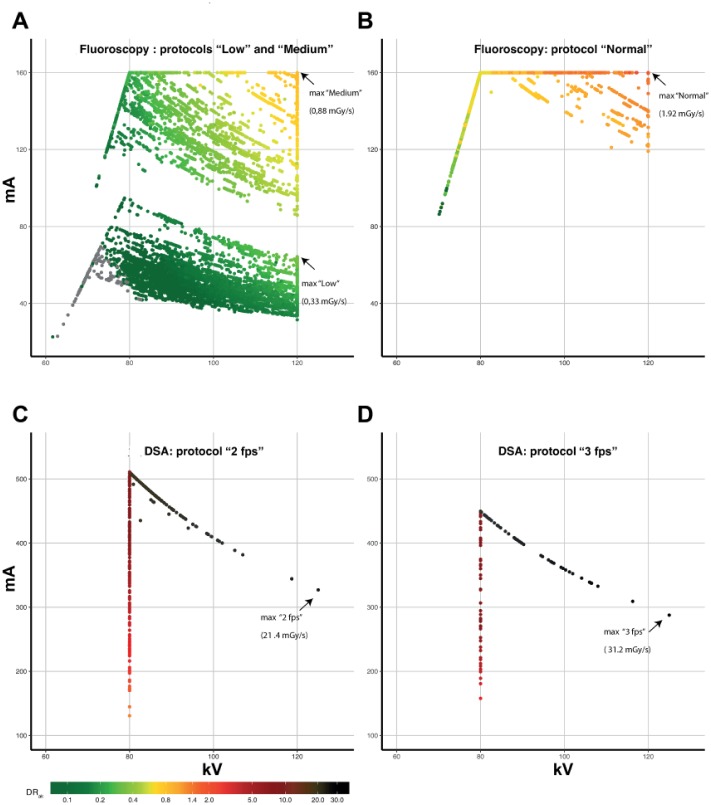
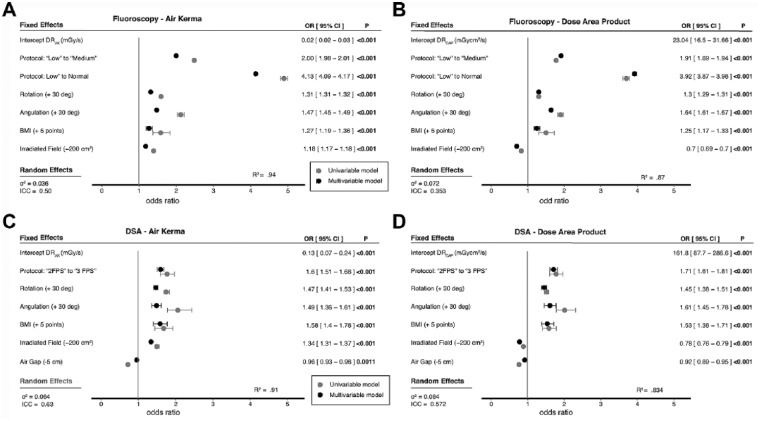
A retrospective analysis was performed of 74 EVAR procedures, including 16,889 X-ray runs using fixed C-arm imaging equipment. Four multivariate log-linear mixed models (with patient as a random effect) were constructed. Mean air kerma DR (DR, mGy/s) and the mean dose area product DR (DR, mGycm/s) were the outcome variables utilized for fluoroscopy as differentiated from digital subtraction angiography (DSA). These models were used to predict the maximum radiation duration allowed before a 2-Gy skin threshold (for DR) or a 500-Gycm threshold (for DR) was reached.
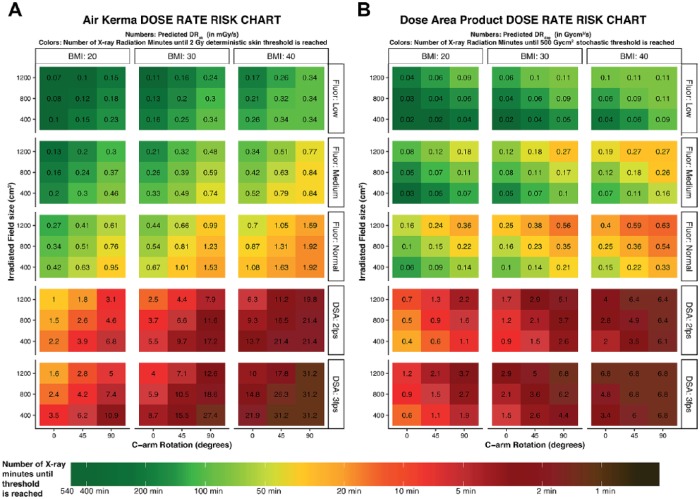
The strongest predictor of DR and DR for fluoroscopy imaging was the radiation protocol, with an increase of 200% when changing from "low" to "medium" and 410% from "low" to "normal." The strongest predictors of DR and DR for DSA were C-arm angulation, with an increase of 47% per 30° of angulation, and body mass index (BMI), with an increase of 58% for every 5-point increase in BMI. Based on these models, a patient with a BMI of 30 kg/m, combined with 45° of rotation and a field size of 800 cm in the medium fluoroscopy protocol has a predicted DR of 0.39 mGy/s (or 85.5 minutes until the 2-Gy skin threshold is reached). While using comparable settings but switching the acquisition to a DSA with a "2 frames per second" protocol, the predicted DR will be 6.6 mGy/s (or 5.0 minutes until the 2-Gy threshold is reached).
X-ray radiation DRs are constantly fluctuating during and between patients based on BMI, the protocols, C-arm position, and the image acquisitions that are used. An instant patient risk chart visualizes these radiation dose fluctuations and provides an overview of the expected duration of X-ray radiation, which can be used to predict when follow-up dose thresholds are reached during abdominal endovascular procedures.
确定在血管内动脉瘤修复(EVAR)手术过程中,哪些患者和C型臂特征是术中患者辐射剂量率(DR)的最强预测因素,并创建患者风险图表。
对74例EVAR手术进行回顾性分析,包括使用固定C型臂成像设备进行的16889次X射线扫描。构建了四个多变量对数线性混合模型(将患者作为随机效应)。平均空气比释动能剂量率(DR,mGy/s)和平均剂量面积乘积剂量率(DR,mGycm/s)是用于荧光透视的结果变量,与数字减影血管造影(DSA)有所区别。这些模型用于预测在达到2 Gy皮肤阈值(针对DR)或500 Gycm阈值(针对DR)之前允许的最大辐射持续时间。
荧光透视成像中DR和DR的最强预测因素是辐射方案,从“低”变为“中”时增加200%,从“低”变为“正常”时增加410%。DSA中DR和DR的最强预测因素是C型臂角度,每30°角度增加47%,以及体重指数(BMI),BMI每增加5点增加58%。基于这些模型,一名BMI为30 kg/m、在中等荧光透视方案中旋转45°且视野大小为800 cm的患者,预测DR为0.39 mGy/s(或在达到2 Gy皮肤阈值前85.5分钟)。在使用类似设置但将采集切换为“每秒2帧”方案的DSA时,预测DR将为6.6 mGy/s(或在达到2 Gy阈值前5.0分钟)。
基于BMI、方案、C型臂位置和使用的图像采集,患者之间及手术过程中X射线辐射DR不断波动。即时患者风险图表可直观显示这些辐射剂量波动,并提供X射线辐射预期持续时间的概述,可用于预测腹部血管内手术中何时达到后续剂量阈值。