Gallagher Hugh, Methven Shona, Casula Anna, Thomas Nicola, Tomson Charles R V, Caskey Fergus J, Rose Tracey, Walters Stephen J, Kennedy David, Dawnay Anne, Cassidy Martin, Fluck Richard, Rayner Hugh C, Nation Michael
South West Thames Renal Unit, Epsom and St Helier NHS Trust, Carshalton, UK.
UK Renal Registry, Bristol, UK.
BMC Nephrol. 2017 Apr 11;18(1):131. doi: 10.1186/s12882-017-0522-9.
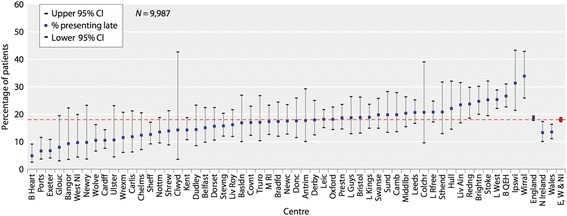
Patients who start renal replacement therapy (RRT) for End-Stage Kidney Disease (ESKD) without having had timely access to specialist renal services have poor outcomes. At one NHS Trust in England, a community-wide CKD management system has led to a decline in the incident rate of RRT and the lowest percentage of patients presenting within 90 days of starting RRT in the UK. We describe the protocol for a quality improvement project to scale up and evaluate this innovation.
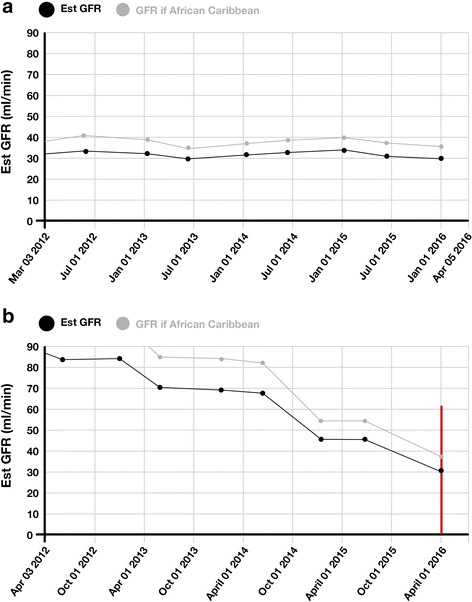
The intervention is based upon an off-line database that integrates laboratory results from blood samples taken in all settings stored under different identifying labels relating to the same patient. Graphs of estimated glomerular filtration rate (eGFR) over time are generated for patients <65 years with an incoming eGFR <50 ml/min/1.73 m and patients >65 years with an incoming eGFR <40 ml/min/1.73 m. Graphs where kidney function is deteriorating are flagged by a laboratory scientist and details sent to the primary care doctor (GP) with a prompt that further action may be needed. We will evaluate the impact of implementing this intervention across a large population served by a number of UK renal centres using a mixed methods approach. We are following a stepped-wedge design. The order of implementation among participating centres will be randomly allocated. Implementation will proceed with unidirectional steps from control group to intervention group until all centres are generating graphs of eGFR over time. The primary outcome for the quantitative evaluation is the proportion of patients referred to specialist renal services within 90 days of commencing RRT, using data collected routinely by the UK Renal Registry. The qualitative evaluation will investigate facilitators and barriers to adoption and spread of the intervention. It will include: semi-structured interviews with laboratory staff, renal centre staff and service commissioners; an online survey of GPs receiving the intervention; and focus groups of primary care staff.
Late presentation to nephrology for patients with ESKD is a source of potentially avoidable harm. This protocol describes a robust quantitative and qualitative evaluation of a quality improvement intervention to reduce late presentation and improve the outcomes for patients with ESKD.
对于终末期肾病(ESKD)患者,如果在开始肾脏替代治疗(RRT)之前未能及时获得专科肾脏服务,其治疗效果较差。在英格兰的一家国民健康服务信托机构,一个全社区范围的慢性肾脏病(CKD)管理系统已使RRT的发病率有所下降,且在英国,在开始RRT后90天内就诊的患者比例达到最低。我们描述了一项质量改进项目的方案,以扩大规模并评估这一创新举措。
该干预措施基于一个离线数据库,该数据库整合了在所有场所采集的血样的实验室检测结果,这些血样以与同一患者相关的不同识别标签存储。为65岁以下且初始估算肾小球滤过率(eGFR)<50ml/min/1.73m²的患者以及65岁以上且初始eGFR<40ml/min/1.73m²的患者生成eGFR随时间变化的图表。肾功能恶化的图表由实验室科学家标记,并将详细信息发送给初级保健医生(全科医生),同时提示可能需要进一步采取行动。我们将采用混合方法评估在英国多个肾脏中心服务的大量人群中实施该干预措施的影响。我们采用阶梯式楔形设计。参与中心的实施顺序将随机分配。实施将从对照组向干预组单向推进,直至所有中心都能生成eGFR随时间变化的图表。定量评估的主要结果是使用英国肾脏登记处常规收集的数据,计算开始RRT后90天内转诊至专科肾脏服务的患者比例。定性评估将调查干预措施采用和推广的促进因素及障碍。这将包括:对实验室工作人员、肾脏中心工作人员和服务专员进行半结构化访谈;对接受干预的全科医生进行在线调查;以及组织初级保健工作人员焦点小组讨论。
ESKD患者延迟就诊是潜在可避免伤害的一个来源。本方案描述了一项对质量改进干预措施进行的有力的定量和定性评估,该干预措施旨在减少延迟就诊并改善ESKD患者的治疗效果。