Spina Tensini Fernando, Sato Mario T, Shiokawa Naoye, Ashizawa Tetsuo, Teive Hélio A G
Movement Disorders Unit, Neurology Service, Internal Medicine Department, Hospital de Clínicas, Federal University of Paraná, Rua Treze de Maio, 200, apto 103, Centro, Curitiba, PR, CEP 80020-270, Brazil.
Neuro-Ophthalmology and Ocular Electrophysiology Sector, Vision Center, Hospital de Clínicas, Federal University of Paraná, Curitiba, PR, Brazil.
Cerebellum. 2017 Aug;16(4):797-801. doi: 10.1007/s12311-017-0856-7.
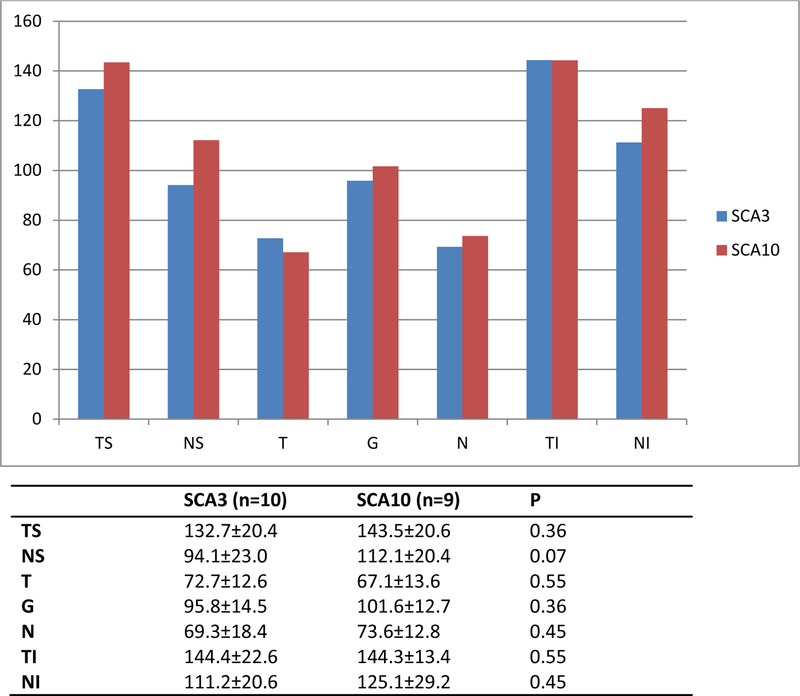
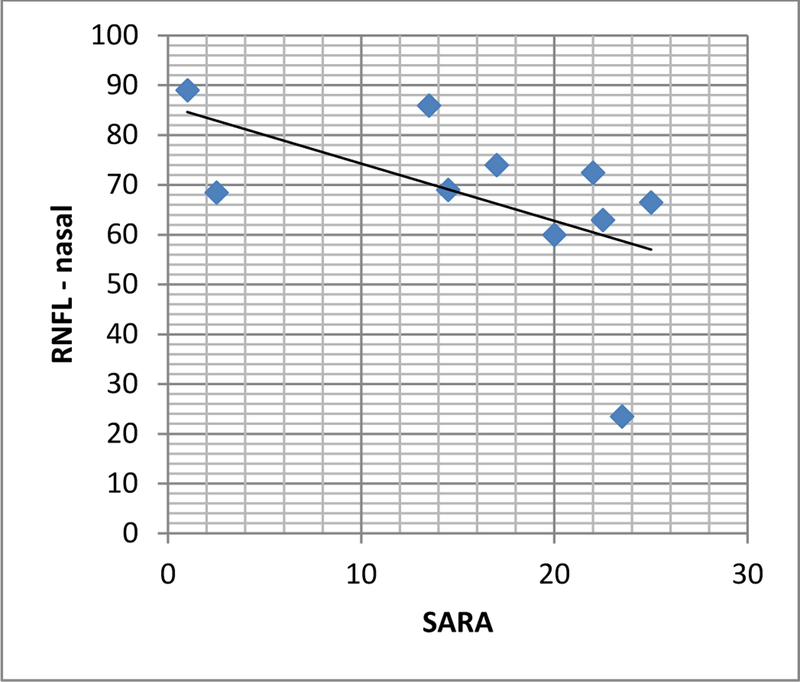
SCA3 presents with a CAG expansion at 14q24.3-q32 while SCA10 shows an ATTCT expansion at 22q13-qter. SCA10 seems to be less aggressive than SCA3. For an in vivo, noninvasive approach of the correlation between central nervous system and clinical evolution, we can use optic coherence tomography (OCT) to measure retinal nerve fiber (RNFL) and ganglion cell layer (GCL) thickness. To describe OCT findings in SCA10, correlate it with expansion size and disease severity and compare with those of SCA3. We analyzed ten individuals with SCA3 and nine with SCA10 recruited from the neurology service of Hospital de Clínicas of Paraná-Brazil. They were submitted to OCT and clinical evaluation using SARA score. Expansion size, demographic data, time from disease onset, and age of onset were collected. We found no correlation between size of expansion, SARA, and RNFL or GCL thickness in SCA10. RNFL seemed to be thicker in SCA10 (p > 0.05). GCL thickness, SARA, median age, and time from disease onset did not differ between groups. SCA10 individuals had an earlier disease onset. In SCA3, there was a negative correlation between SARA and RNFL thickness in nasal area. To the best of our knowledge, this is the first paper assessing retinal changes by OCT in individuals with SCA10. The lack of correlation between disease progression, age, and time since onset supports the anatomopathological findings which suggest SCA10 is less aggressive than other SCAs. The findings in SCA3 are in accordance with the literature.
脊髓小脑共济失调3型(SCA3)表现为14q24.3 - q32处的CAG重复序列扩增,而脊髓小脑共济失调10型(SCA10)则显示22q13 - qter处的ATTCT重复序列扩增。SCA10似乎比SCA3的侵袭性小。为了采用一种体内非侵入性方法研究中枢神经系统与临床进展之间的相关性,我们可以使用光学相干断层扫描(OCT)来测量视网膜神经纤维层(RNFL)和神经节细胞层(GCL)的厚度。为了描述SCA10患者的OCT检查结果,将其与重复序列扩增大小和疾病严重程度相关联,并与SCA3患者的结果进行比较。我们分析了从巴西巴拉那州临床医院神经科招募的10例SCA3患者和9例SCA10患者。他们接受了OCT检查,并使用共济失调评定量表(SARA)进行临床评估。收集了重复序列扩增大小、人口统计学数据、疾病发病时间和发病年龄。我们发现SCA10患者的重复序列扩增大小、SARA评分与RNFL或GCL厚度之间无相关性。SCA10患者的RNFL似乎更厚(p > 0.05)。两组之间的GCL厚度、SARA评分、中位年龄和疾病发病时间无差异。SCA10患者的发病年龄较早。在SCA3患者中,SARA评分与鼻侧RNFL厚度呈负相关。据我们所知,这是第一篇评估SCA10患者视网膜变化的OCT研究论文。疾病进展、年龄和发病时间之间缺乏相关性,支持了解剖病理学研究结果,即SCA10比其他脊髓小脑共济失调的侵袭性小。SCA3的研究结果与文献一致。