Tsuzuki Ippei, Iigaya Kamon, Matsubara Takashi, Takagi Shunsuke, Inohara Taku, Ohgino Yasuyuki, Imafuku Toshio
Department of Internal Medicine, Hiratsuka city Hospital, 1-19-1 Minamihara, Hiratsuka city, Kanagawa, 254-0065, Japan.
Department of Cardiology, Hiratsuka city Hospital, 1-19-1 Minamihara, Hiratsuka city, Kanagawa, 254-0065, Japan.
J Med Case Rep. 2017 Apr 12;11(1):109. doi: 10.1186/s13256-017-1267-6.
Platypnea-orthodeoxia syndrome is a rare syndrome characterized by dyspnea and hypoxia when the patient is sitting or standing. Here we report a case of platypnea-orthodeoxia syndrome caused by a right hemidiaphragmatic elevation with giant liver cyst that triggered a right-to-left shunt through the patent foramen ovale. This case report is the first presentation of a case secondary to hemidiaphragmatic elevation with giant liver cyst. In addition to this, a malposition of the pacemaker lead could be associated with platypnea-orthodeoxia syndrome in this case.
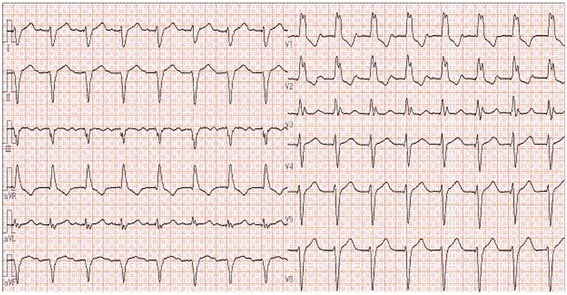
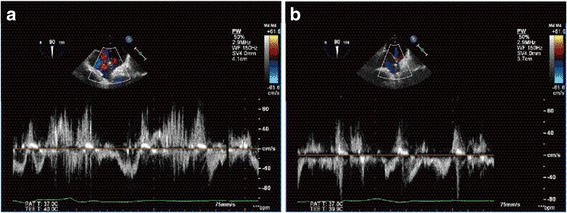
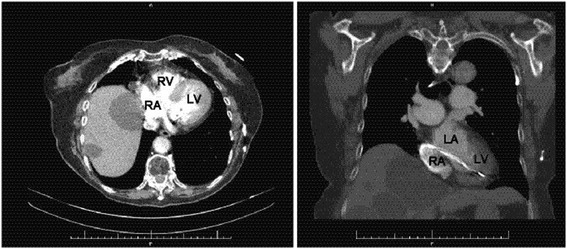
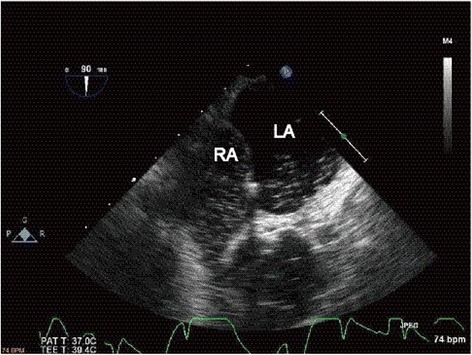
A 91-year-old Japanese woman presented to our hospital with hypoxia of unknown origin. Severe hypoxia and cyanosis were observed only in the right lateral decubitus position. A chest X-ray and computed tomography scan revealed right hemidiaphragmatic elevation, which was probably compressing the right atrium. A transesophageal echocardiogram showed a compressed right atrium and shunt blood flow in both directions: from the left to the right atrium and vice versa. The shunt flow was exacerbated by postural changes from the left to the right lateral decubitus. A transesophageal echocardiogram also confirmed compression of the right atrium due to giant liver cyst and a malposition of the pacemaker lead abnormally placed in the left atrium through patent foramen ovale. We concluded that the cause of hypoxia was platypnea-orthodeoxia syndrome with right-to-left interatrial shunt through patent foramen ovale. Surgical closure of patent foramen ovale was not performed due to the age of our patient, surgical difficulties, and failure to obtain informed consent. For these reasons she was discharged after receiving medical advice about her posture.
Platypnea-orthodeoxia syndrome is rare and difficult to diagnose. The present case suggests that hypoxia due to postural changes should be considered a differential diagnosis of platypnea-orthodeoxia syndrome.
平卧呼吸-直立性低氧血症综合征是一种罕见的综合征,其特征为患者在坐位或站立位时出现呼吸困难和低氧血症。在此,我们报告一例由右半膈肌抬高伴巨大肝囊肿引起的平卧呼吸-直立性低氧血症综合征,该综合征通过卵圆孔未闭引发了右向左分流。本病例报告是首例因半膈肌抬高伴巨大肝囊肿继发的病例。除此之外,在该病例中起搏器导线位置异常可能与平卧呼吸-直立性低氧血症综合征有关。
一名91岁的日本女性因不明原因的低氧血症就诊于我院。仅在右侧卧位时观察到严重的低氧血症和发绀。胸部X线和计算机断层扫描显示右半膈肌抬高,可能压迫右心房。经食管超声心动图显示右心房受压,且存在双向分流:从左心房到右心房,反之亦然。从左侧卧位到右侧卧位的体位改变会使分流加剧。经食管超声心动图还证实了巨大肝囊肿导致右心房受压,以及起搏器导线通过卵圆孔未闭异常地置于左心房。我们得出结论,低氧血症的原因是平卧呼吸-直立性低氧血症综合征伴通过卵圆孔未闭的右向左心房分流。由于患者年龄、手术难度以及未能获得知情同意,未进行卵圆孔未闭的手术闭合。由于这些原因,她在接受关于体位的医学建议后出院。
平卧呼吸-直立性低氧血症综合征罕见且难以诊断。本病例提示,因体位改变导致的低氧血症应被视为平卧呼吸-直立性低氧血症综合征的鉴别诊断。