Klaman Stacey L, Isaacs Krystyna, Leopold Anne, Perpich Joseph, Hayashi Susan, Vender Jeff, Campopiano Melinda, Jones Hendrée E
Department of Maternal and Child Health, University of North Carolina at Chapel Hill Gillings School of Global Public Health, Chapel Hill, NC (SLK); JBS International, Inc., North Bethesda, MD (KI, AL, JP, SH, JV); Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services, Rockville, MD (MC); UNC Horizons, Department of Obstetrics and Gynecology, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC (HEJ); Departments of Psychiatry and Behavioral Sciences and Obstetrics and Gynecology, School of Medicine, Johns Hopkins University, Baltimore, MD (HEJ).
J Addict Med. 2017 May/Jun;11(3):178-190. doi: 10.1097/ADM.0000000000000308.
The prevalence of opioid use disorder (OUD) during pregnancy is increasing. Practical recommendations will help providers treat pregnant women with OUD and reduce potentially negative health consequences for mother, fetus, and child. This article summarizes the literature review conducted using the RAND/University of California, Los Angeles Appropriateness Method project completed by the US Department of Health and Human Services Substance Abuse and Mental Health Services Administration to obtain current evidence on treatment approaches for pregnant and parenting women with OUD and their infants and children.
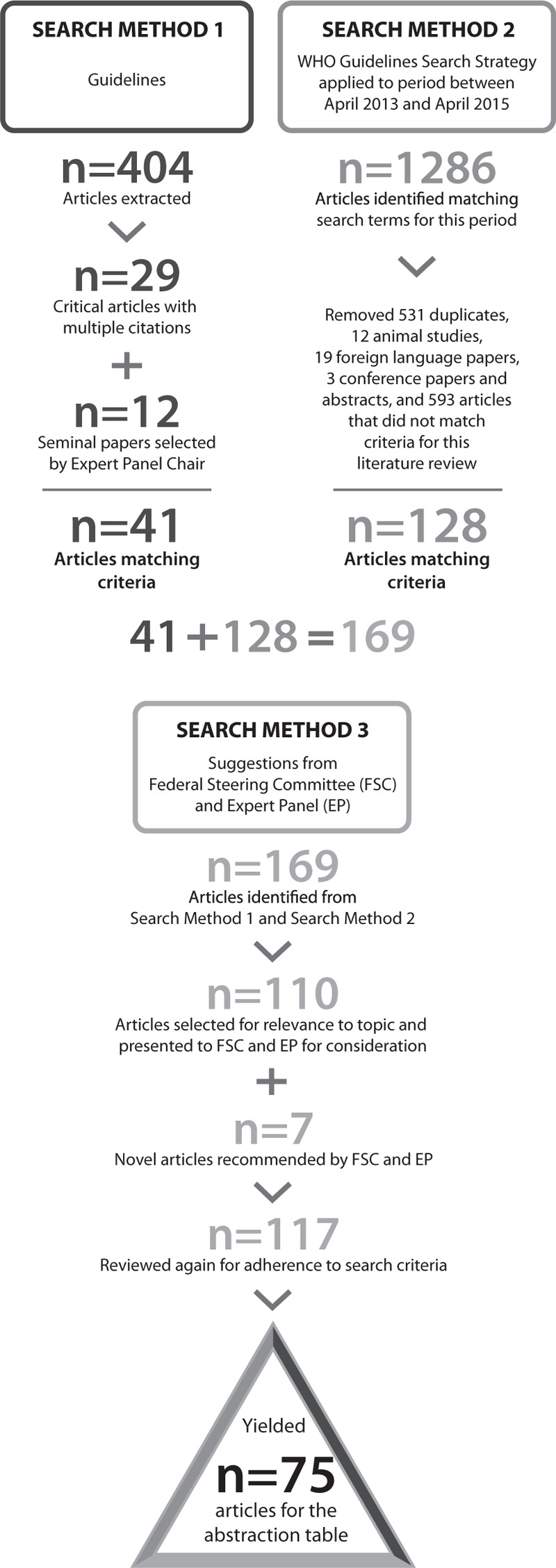
Three separate search methods were employed to identify peer-reviewed journal articles providing evidence on treatment methods for women with OUD who are pregnant or parenting, and for their children. Identified articles were reviewed for inclusion per study guidelines and relevant information was abstracted and summarized.
Of the 1697 articles identified, 75 were included in the literature review. The perinatal use of medication for addiction treatment (MAT, also known as medication-assisted treatment), either methadone or buprenorphine, within comprehensive treatment is the most accepted clinical practice, as withdrawal or detoxification risks relapse and treatment dropout. Medication increases may be needed with advancing pregnancy, and are not associated with more severe neonatal abstinence syndrome (NAS). Switching medication prenatally is usually not recommended as it can destabilize opioid abstinence. Postnatally, breastfeeding is seen as beneficial for the infant for women who are maintained on a stable dose of opioid agonist medication. Less is known about ideal pain management and postpartum dosing regimens. NAS appears generally less severe following prenatal exposure to buprenorphine versus methadone. Frontline NAS medication treatments include protocol-driven methadone and morphine dosing in the context of nonpharmacological supports.
Women with OUD can be treated with methadone or buprenorphine during pregnancy. NAS is an expected and manageable condition. Although research has substantially advanced, opportunities to guide future research to improve maternal and infant outcomes are provided.
孕期阿片类物质使用障碍(OUD)的患病率正在上升。实用的建议将有助于医疗服务提供者治疗患有OUD的孕妇,并减少对母亲、胎儿和儿童潜在的负面健康影响。本文总结了美国卫生与公众服务部药物滥用和精神健康服务管理局完成的使用兰德/加利福尼亚大学洛杉矶分校适宜性方法项目进行的文献综述,以获取关于患有OUD的孕妇及其婴儿和儿童治疗方法的当前证据。
采用三种不同的检索方法来识别经同行评审的期刊文章,这些文章提供了关于患有OUD的孕妇及其子女治疗方法的证据。根据研究指南对识别出的文章进行纳入审查,并提取和总结相关信息。
在识别出的1697篇文章中,75篇被纳入文献综述。在综合治疗中,围产期使用药物辅助治疗成瘾(MAT,也称为药物辅助治疗),即美沙酮或丁丙诺啡,是最被认可的临床实践,因为戒断或脱毒有复发和治疗中断的风险。随着孕周增加可能需要增加药物剂量,且与更严重的新生儿戒断综合征(NAS)无关。通常不建议在产前更换药物,因为这可能会破坏阿片类物质戒断状态。产后,对于维持稳定剂量阿片类激动剂药物的女性,母乳喂养对婴儿有益。关于理想的疼痛管理和产后给药方案知之甚少。与美沙酮相比,产前接触丁丙诺啡后NAS通常不太严重。一线NAS药物治疗包括在非药物支持的情况下按方案使用美沙酮和吗啡给药。
患有OUD的女性在孕期可以用美沙酮或丁丙诺啡治疗。NAS是一种可预期且可控制的情况。尽管研究有了很大进展,但仍提供了指导未来研究以改善母婴结局的机会。