Karl Florian M, Holle Rolf, Bals Robert, Greulich Timm, Jörres Rudolf A, Karch Annika, Koch Armin, Karrasch Stefan, Leidl Reiner, Schulz Holger, Vogelmeier Claus, Wacker Margarethe E
Institute of Health Economics and Health Care Management, Helmholtz Zentrum München, GmbH, German Research Center for Environmental Health, Comprehensive Pneumology Center Munich (CPC-M), Member of the German Center for Lung Research, Ingolstaedter Landstr. 1, 85764, Neuherberg, Germany.
Institute for Medical Information Processing Biometrics and Epidemiology (IBE) Ludwig-Maximilians-Universität München (LMU), Marchioninistr. 15, 81377, Munich, Germany.
Respir Res. 2017 Apr 17;18(1):60. doi: 10.1186/s12931-017-0543-8.
Alpha-1-Antitrypsin Deficiency (AATD) is an economically unexplored genetic disease.
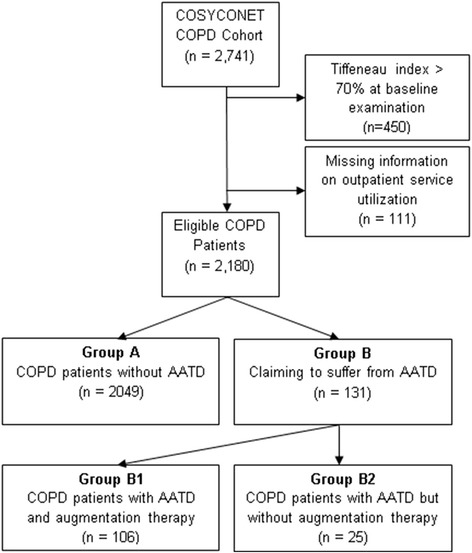
Direct and indirect costs (based on self-reported information on healthcare utilization) and health-related quality of life (HRQL, as assessed by SGRQ, CAT, and EQ-5D-3 L) were compared between 131 AATD patients (106 with, 25 without augmentation therapy (AT)) and 2,049 COPD patients without AATD participating in the COSYCONET COPD cohort. The medication costs of AT were excluded from all analyses to reveal differences associated with morbidity profiles. The association of AATD (with/without AT) with costs or HRQL was examined using generalized linear regression modelling (GLM) adjusting for age, sex, GOLD grade, BMI, smoking status, education and comorbidities.
Adjusted mean direct annual costs were €6,099 in AATD patients without AT, €7,117 in AATD patients with AT (excluding costs for AT), and €7,460 in COPD patients without AATD. AATD with AT was significantly associated with higher outpatient (+273%) but lower inpatient (-35%) and medication costs (-10%, disregarding AT) compared with COPD patients without AATD. There were no significant differences between groups regarding indirect costs and HRQL.
Apart from AT costs, AATD patients tended to have lower, though not significant, overall costs and similar HRQL compared to COPD patients without AATD. AT was not associated with lower costs or higher HRQL.
NCT01245933.
α-1抗胰蛋白酶缺乏症(AATD)是一种在经济方面尚未得到充分研究的遗传病。
比较了131例AATD患者(106例接受、25例未接受增强治疗(AT))与参与COSYCONET慢性阻塞性肺疾病(COPD)队列研究的2049例无AATD的COPD患者的直接和间接费用(基于自我报告的医疗保健利用信息)以及健康相关生活质量(HRQL,通过圣乔治呼吸问卷(SGRQ)、慢阻肺评估测试(CAT)和欧洲五维度健康量表(EQ-5D-3L)进行评估)。在所有分析中均排除了AT的药物费用,以揭示与发病情况相关的差异。使用广义线性回归模型(GLM)对年龄、性别、慢性阻塞性肺疾病全球倡议(GOLD)分级、体重指数(BMI)、吸烟状况、教育程度和合并症进行调整,研究AATD(有/无AT)与费用或HRQL之间的关联。
未接受AT的AATD患者调整后的年均直接费用为6099欧元,接受AT的AATD患者(不包括AT费用)为7117欧元,无AATD的COPD患者为7460欧元。与无AATD的COPD患者相比,接受AT的AATD患者门诊费用显著更高(增加273%),但住院费用(降低35%)和药物费用更低(降低10%,不考虑AT)。各组之间在间接费用和HRQL方面无显著差异。
除AT费用外,与无AATD的COPD患者相比,AATD患者的总体费用往往较低(但不显著),且HRQL相似。AT与较低费用或较高HRQL无关。
NCT01245933。