Reichetzeder Christoph, von Websky Karoline, Tsuprykov Oleg, Mohagheghi Samarin Azadeh, Falke Luise Gabriele, Dwi Putra Sulistyo Emantoko, Hasan Ahmed Abdallah, Antonenko Viktoriia, Curato Caterina, Rippmann Jörg, Klein Thomas, Hocher Berthold
Institute of Nutritional Science, University of Potsdam, Nuthetal, Germany.
Center for Cardiovascular Research, Charité - Universitätsmedizin Berlin, Berlin, Germany.
Br J Pharmacol. 2017 Jul;174(14):2273-2286. doi: 10.1111/bph.13822. Epub 2017 Jun 7.
Results regarding protective effects of dipeptidyl peptidase 4 (DPP4) inhibitors in renal ischaemia-reperfusion injury (IRI) are conflicting. Here we have compared structurally unrelated DPP4 inhibitors in a model of renal IRI.
IRI was induced in uninephrectomized male rats by renal artery clamping for 30 min. The sham group was uninephrectomized but not subjected to IRI. DPP4 inhibitors or vehicle were given p.o. once daily on three consecutive days prior to IRI: linagliptin (1.5 mg·kg ·day ), vildagliptin (8 mg·kg ·day ) and sitagliptin (30 mg·kg ·day ). An additional group received sitagliptin until study end (before IRI: 30 mg·kg ·day ; after IRI: 15 mg·kg ·day ).
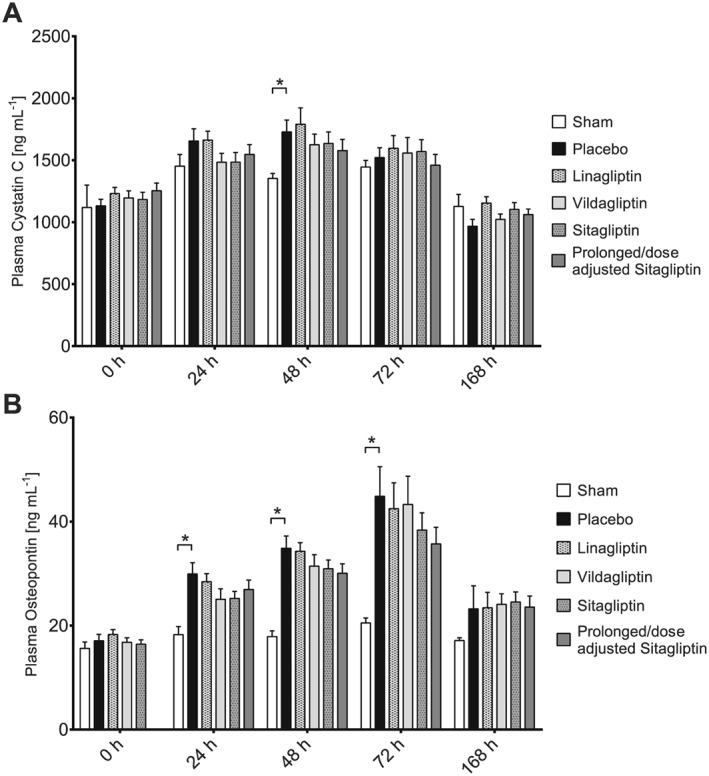
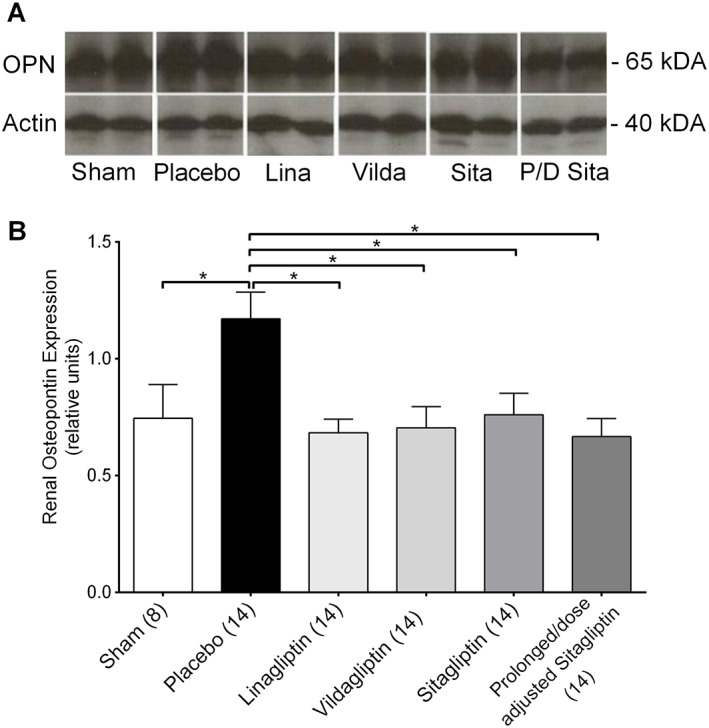
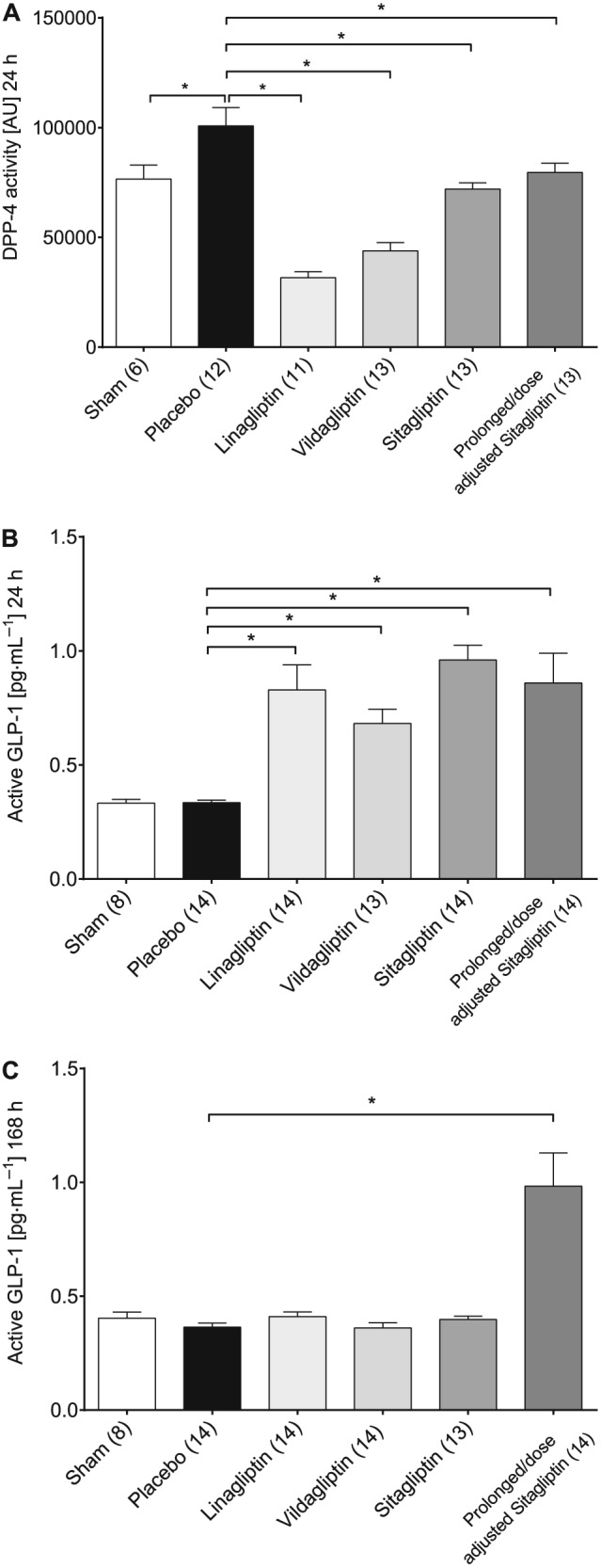
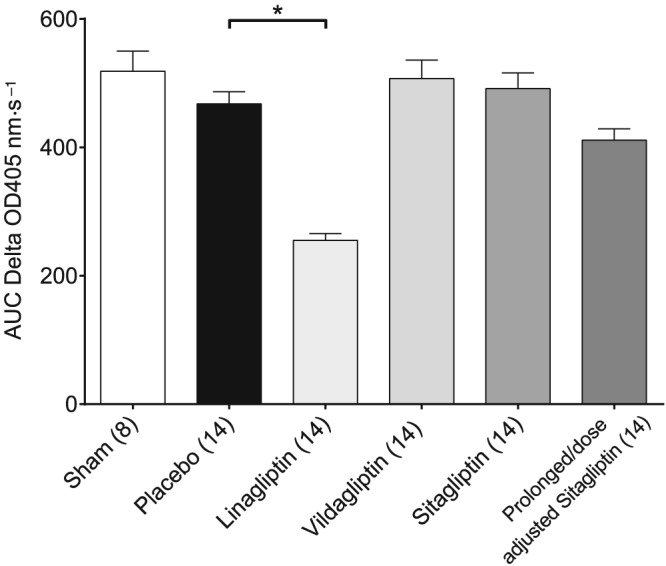
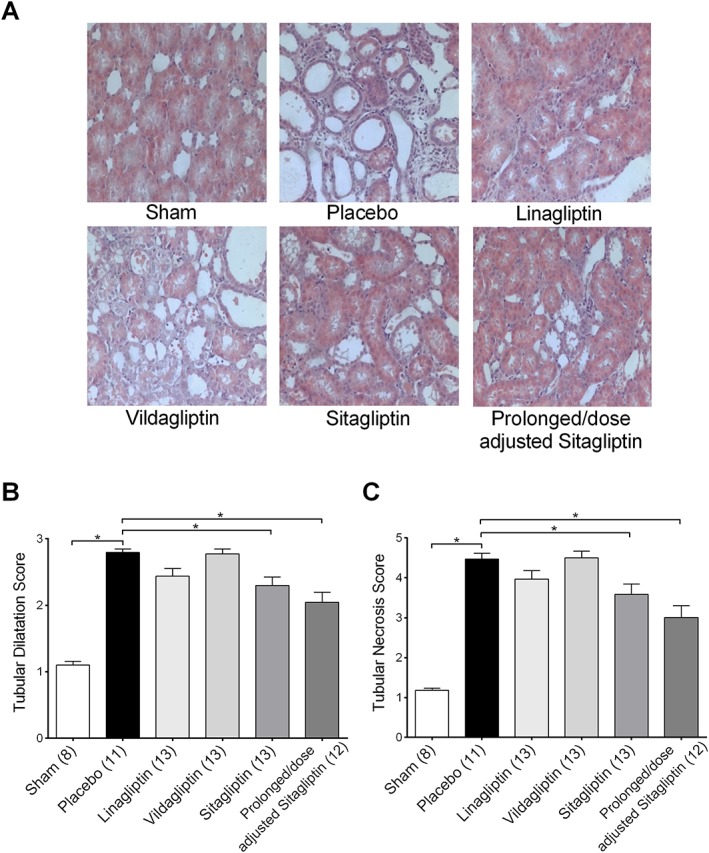
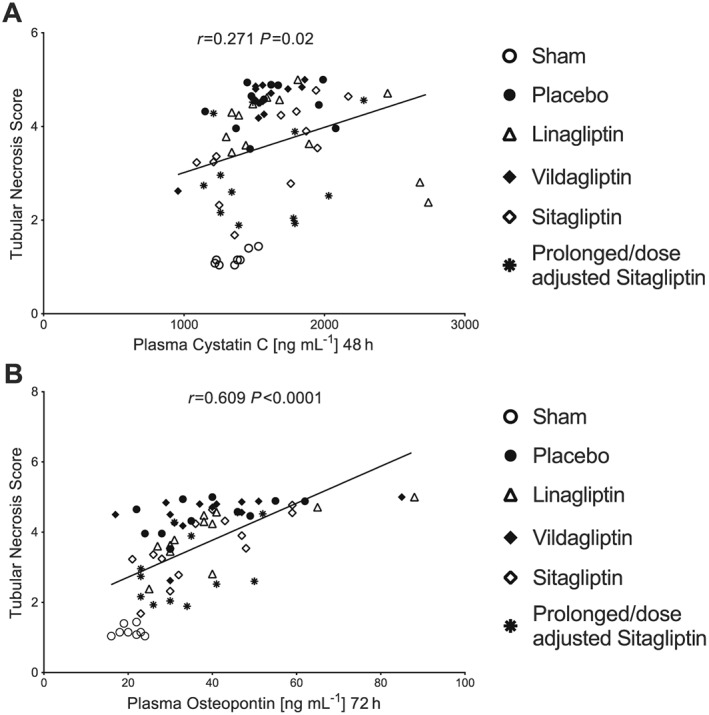
Plasma-active glucagon-like peptide type 1 (GLP-1) increased threefold to fourfold in all DPP4 inhibitor groups 24 h after IRI. Plasma cystatin C, a marker of GFR, peaked 48 h after IRI. Compared with the placebo group, DPP4 inhibition did not reduce increased plasma cystatin C levels. DPP4 inhibitors ameliorated histopathologically assessed tubular damage with varying degrees of drug-specific efficacies. Renal osteopontin expression was uniformly reduced by all DPP4 inhibitors. IRI-related increased renal cytokine expression was not decreased by DPP4 inhibition. Renal DPP4 activity at study end was significantly inhibited in the linagliptin group, but only numerically reduced in the prolonged/dose-adjusted sitagliptin group. Active GLP-1 plasma levels at study end were increased only in the prolonged/dose-adjusted sitagliptin treatment group.
In rats with renal IRI, DPP4 inhibition did not alter plasma cystatin C, a marker of glomerular function, but may protect against tubular damage.
关于二肽基肽酶4(DPP4)抑制剂在肾缺血再灌注损伤(IRI)中的保护作用,研究结果存在矛盾。在此,我们在肾IRI模型中比较了结构不相关的DPP4抑制剂。
通过夹闭肾动脉30分钟,在单侧肾切除的雄性大鼠中诱导IRI。假手术组进行了单侧肾切除,但未进行IRI。在IRI前连续三天每天口服给予DPP4抑制剂或赋形剂:利格列汀(1.5毫克·千克·天)、维格列汀(8毫克·千克·天)和西格列汀(30毫克·千克·天)。另一组在研究结束前持续给予西格列汀(IRI前:30毫克·千克·天;IRI后:15毫克·千克·天)。
IRI后24小时,所有DPP4抑制剂组的血浆活性胰高血糖素样肽-1(GLP-1)增加了三倍至四倍。血浆胱抑素C(肾小球滤过率的标志物)在IRI后48小时达到峰值。与安慰剂组相比,DPP4抑制并未降低血浆胱抑素C升高的水平。DPP4抑制剂改善了经组织病理学评估的肾小管损伤,且具有不同程度的药物特异性疗效。所有DPP4抑制剂均使肾骨桥蛋白表达一致降低。DPP4抑制并未降低IRI相关的肾细胞因子表达增加。研究结束时,利格列汀组的肾DPP4活性受到显著抑制,但在延长/调整剂量的西格列汀组中仅出现数值上的降低。仅在延长/调整剂量的西格列汀治疗组中,研究结束时活性GLP-1血浆水平升高。
在肾IRI大鼠中,DPP4抑制并未改变作为肾小球功能标志物的血浆胱抑素C,但可能预防肾小管损伤。