Roche Lisa M, Niu Xiaoling, Stroup Antoinette M, Henry Kevin A
Cancer Epidemiology Services, New Jersey Department of Health, Trenton, New Jersey (Dr Roche and Ms Niu); Division of Cancer Epidemiology, Rutgers School of Public Health and Rutgers Cancer Institute of New Jersey, New Brunswick, New Jersey (Dr Stroup); Department of Geography and Urban Studies, Temple University, Philadelphia, Pennsylvania (Dr Henry); and Fox Chase Cancer Center, Temple University Health System, Philadelphia, Pennsylvania (Dr Henry).
J Public Health Manag Pract. 2017 Sep/Oct;23(5):477-486. doi: 10.1097/PHH.0000000000000524.
Despite improvements in early detection of breast cancer, disparities persist in stage at diagnosis, which is an important prognostic factor.
We used the space-time scan statistic in SaTScan to identify geographic areas and time periods with significantly elevated proportions of female breast cancer diagnosed at the in situ or distant stage in New Jersey. The analyses were conducted with census tracts as the geographic unit of analysis, elliptical spatial windows, 3-year temporal windows, and Poisson models. Statistical significance was determined by 999 Monte Carlo simulations (P < .05); significant clusters were mapped in ArcMap. Breast cancer cases within the clusters were compared with breast cancer cases outside the clusters on demographic, socioeconomic, and clinical factors using the Pearson chi-square test (P < .05). In addition, populations within the clusters were compared with the population outside the clusters on demographic and socioeconomic factors.
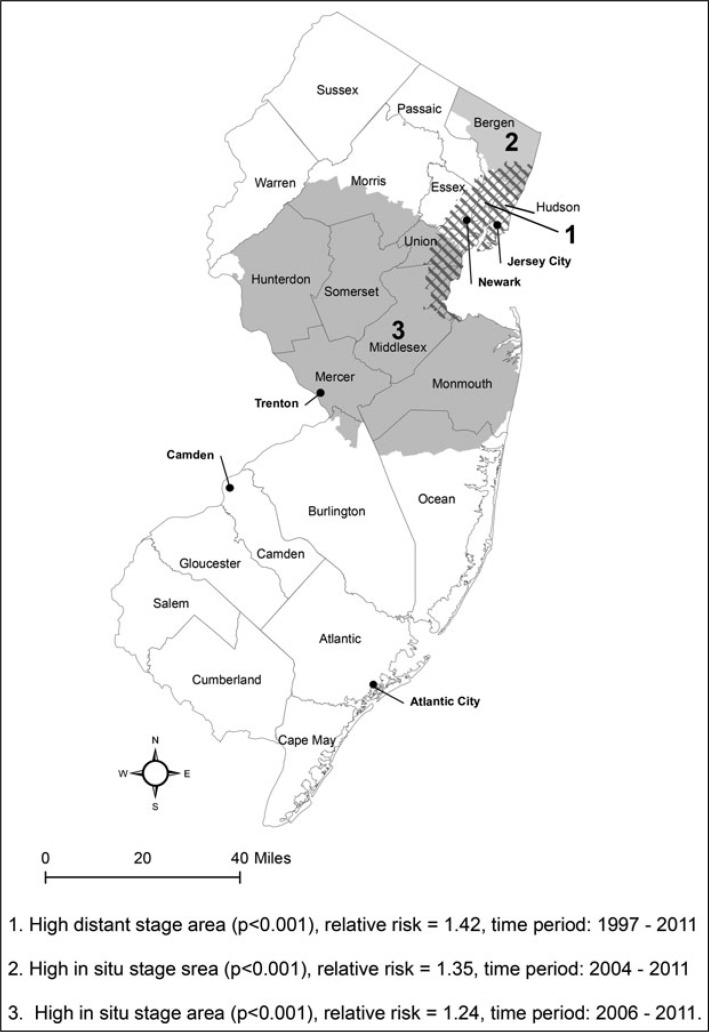
After exclusions, 126 756 cases of primary female breast cancer diagnosed in 1997 to 2011 from the New Jersey State Cancer Registry were included in the analysis. One distant stage breast cancer cluster was identified in northeastern New Jersey from 1997 through 2011 (n = 26 244, relative risk [RR] = 1.42, P < .001). Two in situ breast cancer clusters were found in northeastern New Jersey from 2004 through 2011 (n = 12 496, RR = 1.35, P < .001) and in central New Jersey from 2006 through 2011 (n = 29 319, RR = 1.24, P < .001). The distant stage cluster contained relatively high percentages of minority and lower socioeconomic status (SES) breast cancer cases and populations, whereas the in situ clusters had relatively low percentages of minority and lower SES breast cancer cases and populations.
Although there have been improvements since an earlier study of distant stage breast cancer diagnosed in 1995 to 1997, disparities in stage at diagnosis continue. These findings can be used by our local cancer control partners to target specific populations for interventions such as breast cancer education and mammography screening, as well as by state legislative and public health authorities for resource allocation.
尽管乳腺癌早期检测有所改善,但诊断时的分期差异仍然存在,而分期是一个重要的预后因素。
我们使用时空扫描统计软件SaTScan来识别新泽西州原位或远处分期诊断的女性乳腺癌比例显著升高的地理区域和时间段。分析以普查区为地理分析单位,采用椭圆形空间窗口、3年时间窗口和泊松模型。通过999次蒙特卡罗模拟确定统计学显著性(P <.05);在ArcMap中绘制显著聚类图。使用Pearson卡方检验(P <.05),比较聚类内的乳腺癌病例与聚类外的乳腺癌病例在人口统计学、社会经济和临床因素方面的差异。此外,比较聚类内的人群与聚类外的人群在人口统计学和社会经济因素方面的差异。
排除后,纳入了1997年至2011年新泽西州癌症登记处诊断的126756例原发性女性乳腺癌病例进行分析。1997年至2011年在新泽西州东北部发现1个远处分期乳腺癌聚类(n = 26244,相对风险[RR]=1.42,P <.001)。2004年至2011年在新泽西州东北部发现2个原位乳腺癌聚类(n = 12496,RR = 1.35,P <.001),2006年至2011年在新泽西州中部发现1个原位乳腺癌聚类(n = 29319,RR = 1.24,P <.001)。远处分期聚类中少数族裔和社会经济地位(SES)较低的乳腺癌病例及人群所占百分比相对较高,而原位聚类中少数族裔和SES较低的乳腺癌病例及人群所占百分比相对较低。
尽管自早期对1995年至1997年诊断的远处分期乳腺癌研究以来已有改善,但诊断时的分期差异仍然存在。我们当地的癌症控制合作伙伴可利用这些发现,针对特定人群进行干预,如乳腺癌教育和乳房X光筛查,州立法和公共卫生当局也可利用这些发现进行资源分配。