From the Department of Anesthesiology, Emergency and Critical Care Medicine and Karl Landsteiner Institute of Emergency Medicine, General Hospital Wiener Neustadt, Corvinusring 3-5, A 2700, Wiener Neustadt, Austria.
ÖAMTC Air Rescue, Vienna, Austria.
Scand J Trauma Resusc Emerg Med. 2017 Apr 26;25(1):45. doi: 10.1186/s13049-017-0386-9.
Pre-hospital airway management is a major challenge for emergency medical service (EMS) personnel. Despite convincing evidence that the rescuer's qualifications determine efficacy of tracheal intubation, in-hospital airway management training is not mandatory in Austria, and often neglected. Thus we sought to prove that airway management competence of EMS physicians can be established and maintained by a tailored training program.
In this descriptive quality control study we retrospectively evaluated all in- and pre-hospital airway cases managed by EMS physicians who underwent a structured in-hospital training program in anesthesia at General Hospital Wiener Neustadt. Data was obtained from electronic anesthesia and EMS documentation systems.
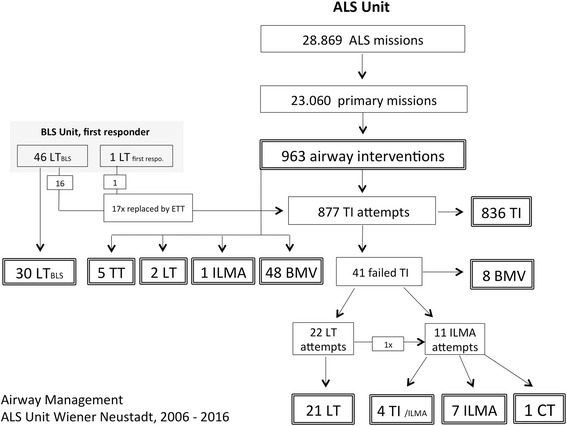
From 2006 to 2016, 32 EMS physicians with 3-year post-graduate education, but without any prior experience in anesthesia were trained. Airway management proficiency was imparted in three steps: initial training, followed by an ongoing practice schedule in the operating room (OR). Median and interquartile range of number of in-hospital tracheal intubations (TIs) vs. use of supra-glottic airway devices (SGA) were 33.5 (27.5-42.5) vs. 19.0 (15.0-27.0) during initial training; 62.0 (41.8-86.5) vs. 33.5 (18.0-54.5) during the first, and 64.0 (34.5-93.8) vs. 27 (12.5-56.0) during the second year. Pre-hospitaly, every physician performed 9.0 (5.0-14.8) TIs vs. 0.0 (0.0-0.0) SGA cases during the first, and 9.0 (7.0-13.8) TIs vs. 0.0 (0.0-0.3) SGA during the second year. Use of an SGA was mandatory when TI failed after the second attempt, thus accounting for a total of 33 cases. In 8 cases, both TI and SGA failed, but bag mask ventilation was successfully performed. No critical events related to airway management were noted and overall success rate for TI with a max of 2 attempts was 95.3%.
Number of TIs per EMS physician is low in the pre-hospital setting. A training concept that assures an additional 60+ TIs per year appears to minimize failure rates. Thus, a fixed amount of working days in anesthesia seems crucial to maintain proficiency. CONCLUSIONS: In-hospital training programs are mandatory for non-anesthetist EMS physicians to gain competence in airway management and emergency anesthesia.Our results might be helpful when discussing the need for regulation and financing with the authorities.
院前气道管理是急救医疗服务(EMS)人员面临的主要挑战。尽管有令人信服的证据表明,救援人员的资质决定了气管插管的效果,但在奥地利,院内气道管理培训并非强制性的,而且往往被忽视。因此,我们试图证明,通过量身定制的培训计划,EMS 医生的气道管理能力可以得到建立和维持。
在这项描述性质量控制研究中,我们回顾性评估了在维也纳新城综合医院接受麻醉院内培训计划的 EMS 医生管理的所有院内和院前气道病例。数据来自电子麻醉和 EMS 文档系统。
2006 年至 2016 年,对 32 名具有 3 年研究生学历但无麻醉经验的 EMS 医生进行了培训。气道管理能力是通过三个步骤传授的:初始培训,然后在手术室(OR)进行持续的实践计划。初始培训时,院内气管插管(TI)中位数和四分位距为 33.5(27.5-42.5)比使用声门上气道装置(SGA)的 19.0(15.0-27.0);第一年为 62.0(41.8-86.5)比 33.5(18.0-54.5),第二年为 64.0(34.5-93.8)比 27(12.5-56.0)。在院前,每位医生进行 9.0(5.0-14.8)次 TI 与 0.0(0.0-0.0)次 SGA 操作,第一年为 0.0(0.0-0.0)次 SGA,第二年为 9.0(7.0-13.8)次 TI 与 0.0(0.0-0.3)次 SGA。第二次尝试失败后,必须使用 SGA 进行 TI,因此总共进行了 33 次操作。在 8 例中,TI 和 SGA 均失败,但成功进行了袋面罩通气。未观察到与气道管理相关的危急事件,TI 最多尝试 2 次的总体成功率为 95.3%。
院前环境中 EMS 医生的 TI 次数较少。一项确保每年额外进行 60 多次 TI 的培训计划似乎可以降低失败率。因此,在麻醉科工作一定数量的工作日对于保持能力至关重要。
非麻醉科 EMS 医生必须接受院内培训计划,以获得气道管理和紧急麻醉方面的能力。我们的结果在与当局讨论监管和融资的必要性时可能会有所帮助。