Department of Anesthesiology and Critical Care, Oslo University Hospital, Ullevål, P.O.Box 4950, Nydalen, N-0424, Oslo, Norway.
Department of Clinical Medicine, University of Oslo, Oslo, Norway.
Scand J Trauma Resusc Emerg Med. 2017 Apr 26;25(1):44. doi: 10.1186/s13049-017-0385-x.
Treatment-limiting decisions (TLD) for severe traumatic brain injury (sTBI) have been sparsely studied. This study determine prevalence, main reason for, categories and timing of TLDs in a Norwegian regional trauma setting.
A retrospective study of a 2-year cohort of 579 sTBI patients admitted to Oslo University Hospital (OUH). Prospectively collected data in the OUH Trauma Registry were combined with retrospective data from a chart review regarding TLDs.
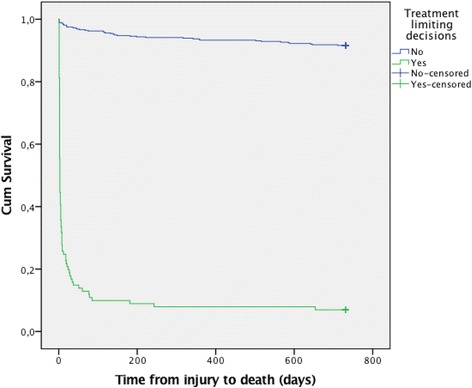
TLDs were documented for 101/579 sTBI patients (17%). The situation was evaluated as futile in 59 cases and as potentially inappropriate in 42 cases. The three most frequent types of TLDs were withholding of neurosurgery, do not resuscitate orders and withdrawing of organ support. In 70% of cases, the first TLD was made within 2 days after injury, while in 14%, the first TLD was made later than day 7. Twenty percent (20/101) of the first TLDs were later adjusted, revoked in 4 patients and broadening of TLDs in 16 patients. The median time from the decision to death was 2 days (range 1-652). TLDs were documented in 93% of in-hospital death cases (n = 79). In-hospital deaths occurred in 73% of TLD group cases and 1% of non-TLD group cases. Family interaction and multi-team discussions were documented in >88% of cases, but no advanced directives were found, and notifications of patients' preferences were found in only 7% of cases.
Clinicians should consider limiting treatment if continued treatment is not in the patients best interest. A range of different types of TLDs were applied for patients after sTBI in the trauma hospital setting.
TLDs were found in 17% of sTBI patients. Value considerations behind TLDs in this care context need to be further explored.
对于严重创伤性脑损伤(sTBI)的治疗限制决策(TLD)研究甚少。本研究旨在确定挪威区域性创伤环境中 TLD 的发生率、主要原因、类别和时间。
对入住奥斯陆大学医院(OUH)的 579 例 sTBI 患者进行了为期 2 年的队列回顾性研究。OUH 创伤登记处前瞻性收集的数据与 TLD 回顾性图表审查数据相结合。
记录了 101/579 例 sTBI 患者(17%)的 TLD。59 例被评估为无效,42 例被评估为可能不适当。三种最常见的 TLD 类型是神经外科手术的回避、不复苏医嘱和器官支持的撤回。70%的情况下,第一次 TLD 在损伤后 2 天内做出,而 14%的情况下,第一次 TLD 在第 7 天以后做出。20%(20/101)的第一次 TLD 后来进行了调整,4 例被撤销,16 例扩大了 TLD。从决定到死亡的中位数时间为 2 天(范围 1-652)。TLD 记录在 93%的院内死亡病例(n=79)中。TLD 组的院内死亡发生率为 73%,非 TLD 组的院内死亡发生率为 1%。在超过 88%的病例中记录了家庭互动和多团队讨论,但未发现预先指示,只有 7%的病例中发现了通知患者偏好的记录。
如果继续治疗不符合患者的最佳利益,临床医生应考虑限制治疗。在创伤医院环境中,对 sTBI 患者应用了一系列不同类型的 TLD。
在 sTBI 患者中发现了 17%的 TLD。需要进一步探讨这种治疗背景下 TLD 背后的价值考虑。