Karapinar-Çarkıt Fatma, van der Knaap Ronald, Bouhannouch Fatiha, Borgsteede Sander D, Janssen Marjo J A, Siegert Carl E H, Egberts Toine C G, van den Bemt Patricia M L A, van Wier Marieke F, Bosmans Judith E
Department of Hospital Pharmacy, OLVG, Amsterdam, The Netherlands.
Department of medication surveillance, Health Base, Houten, The Netherlands.
PLoS One. 2017 Apr 26;12(4):e0174513. doi: 10.1371/journal.pone.0174513. eCollection 2017.
To improve continuity of care at hospital admission and discharge and to decrease medication errors pharmaceutical care programs are developed. This study aims to determine the cost-effectiveness of the COACH program in comparison with usual care from a societal perspective.
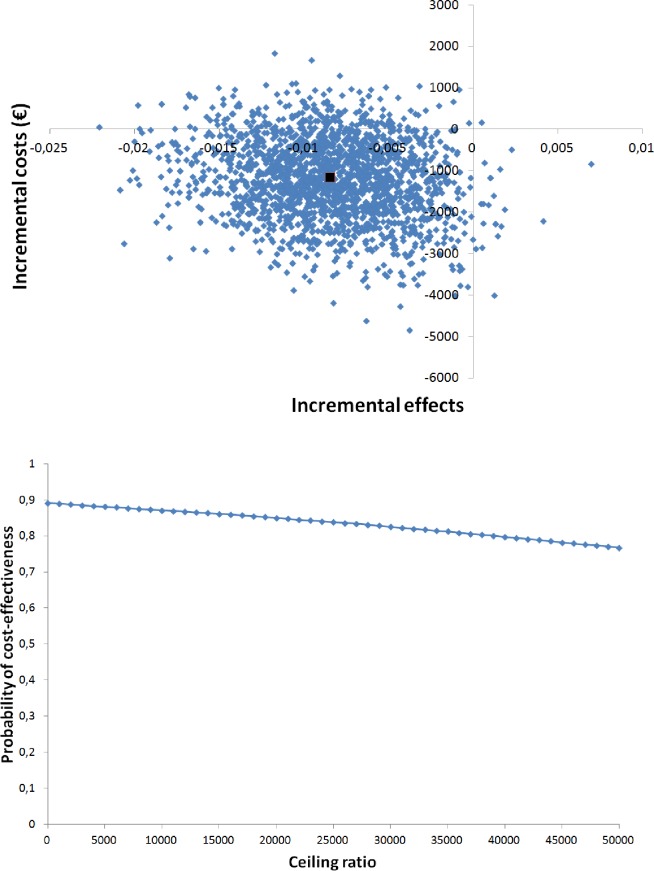
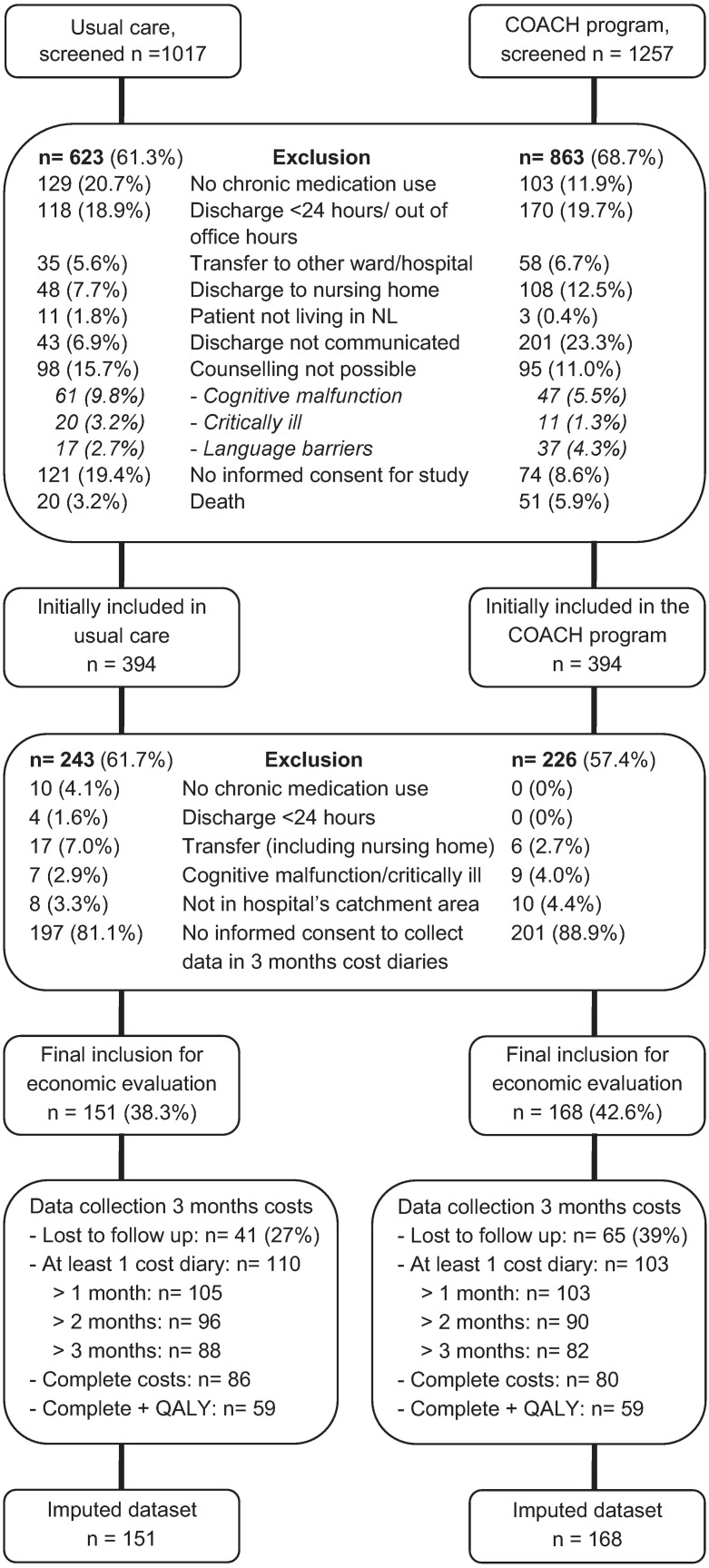
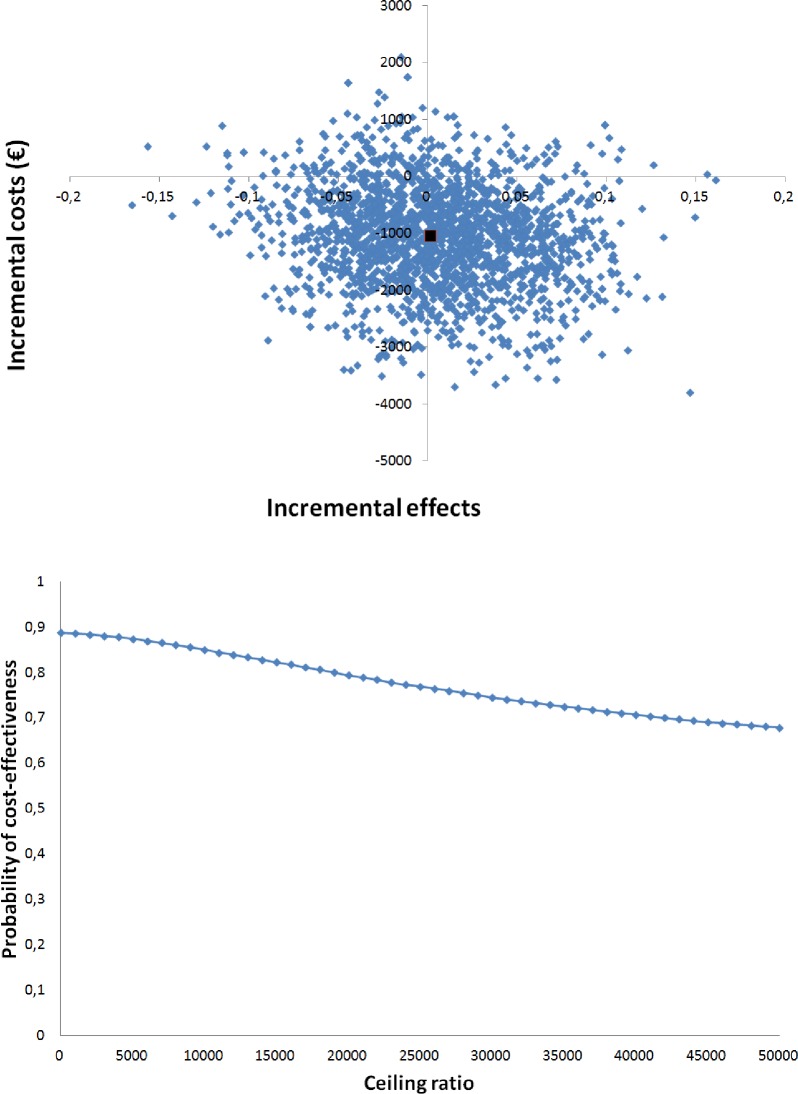
A controlled clinical trial was performed at the Internal Medicine department of a general teaching hospital. All admitted patients using at least one prescription drug were included. The COACH program consisted of medication reconciliation, patient counselling at discharge, and communication to healthcare providers in primary care. The primary outcome was the proportion of patients with an unplanned rehospitalisation within three months after discharge. Also, the number of quality-adjusted life-years (QALYs) was assessed. Cost data were collected using cost diaries. Uncertainty surrounding cost differences and incremental cost-effectiveness ratios between the groups was estimated by bootstrapping.
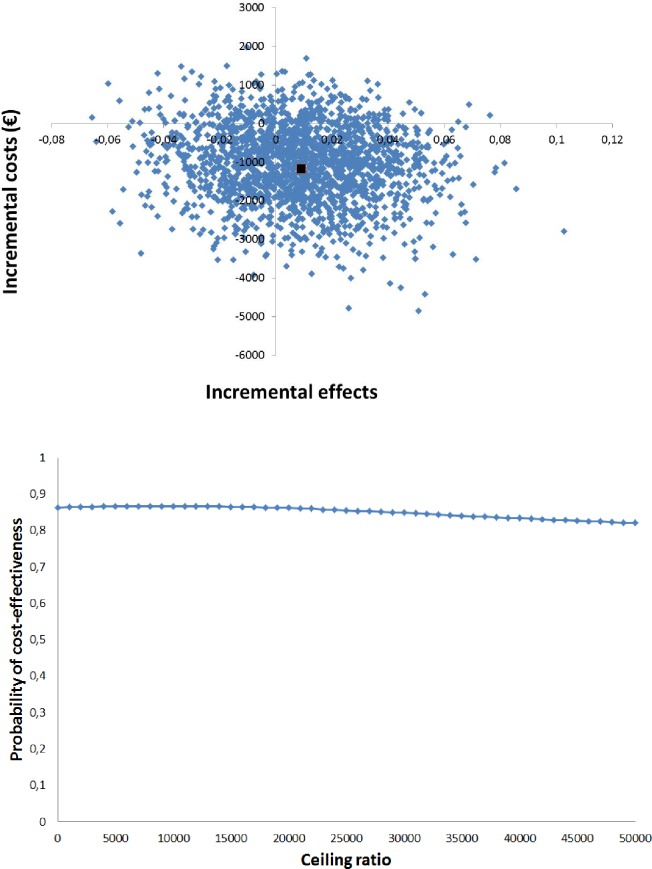
In the COACH program, 168 patients were included and in usual care 151 patients. There was no significant difference in the proportion of patients with unplanned rehospitalisations (mean difference 0.17%, 95% CI -8.85;8.51), and in QALYs (mean difference -0.0085, 95% CI -0.0170;0.0001). Total costs for the COACH program were non-significantly lower than usual care (-€1160, 95% CI -3168;847). Cost-effectiveness planes showed that the program was not cost-effective compared with usual care for unplanned rehospitalisations and QALYs gained.
The COACH program was not cost-effective in comparison with usual care. Future studies should focus on high risk patients and include other outcomes (e.g. adverse drug events) as this may increase the chances of a cost-effective intervention. Dutch trial register NTR1519.
为提高住院和出院时的护理连续性并减少用药错误,制定了药学服务项目。本研究旨在从社会角度确定COACH项目与常规护理相比的成本效益。
在一家普通教学医院的内科进行了一项对照临床试验。纳入所有至少使用一种处方药的住院患者。COACH项目包括用药核对、出院时的患者咨询以及与初级保健中的医疗服务提供者沟通。主要结局是出院后三个月内非计划再次住院患者的比例。此外,还评估了质量调整生命年(QALY)的数量。使用成本日记收集成本数据。通过自抽样估计两组之间成本差异和增量成本效益比的不确定性。
COACH项目纳入了168例患者,常规护理组纳入了151例患者。非计划再次住院患者的比例(平均差异0.17%,95%CI -8.85;8.51)和QALY(平均差异-0.0085,95%CI -0.0170;0.0001)没有显著差异。COACH项目的总成本略低于常规护理,但无统计学意义(-1160欧元,95%CI -3168;847)。成本效益分析表明,与常规护理相比,该项目在非计划再次住院和获得的QALY方面不具有成本效益。
与常规护理相比,COACH项目不具有成本效益。未来的研究应关注高危患者,并纳入其他结局(如药物不良事件),因为这可能增加具有成本效益干预措施的机会。荷兰试验注册编号NTR1519。