D Hayashi Reiko, Yamaoka Masaya, Nishizawa Hitoshi, Fukuda Shiro, Fujishima Yuya, Kimura Takekazu, Kozawa Jyunji, Kita Shunbun, Matsuoka Taka-Aki, Otsuki Michio, Imagawa Akihisa, Ichida Kimiyoshi, Taniguchi Atsuo, Maeda Norikazu, Funahashi Tohru, Shimomura Iichiro
Department of Metabolic Medicine, Graduate School of Medicine, Osaka University, Japan.
Department of Metabolism and Atherosclerosis, Graduate School of Medicine, Osaka University, Japan.
Intern Med. 2017;56(9):1071-1077. doi: 10.2169/internalmedicine.56.7923. Epub 2017 May 1.
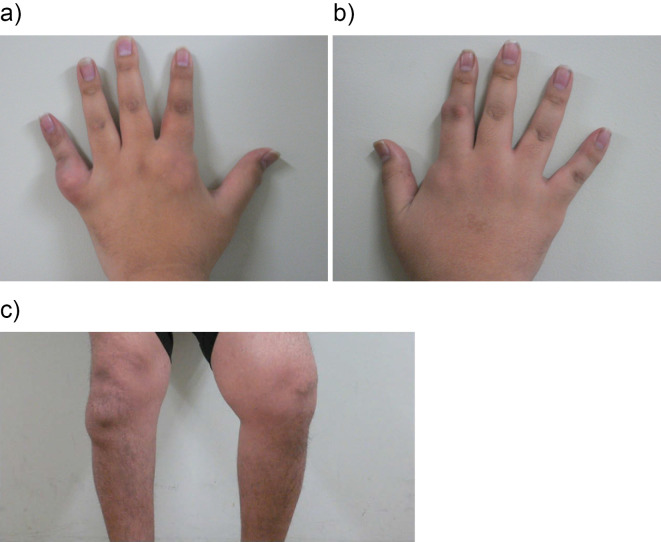
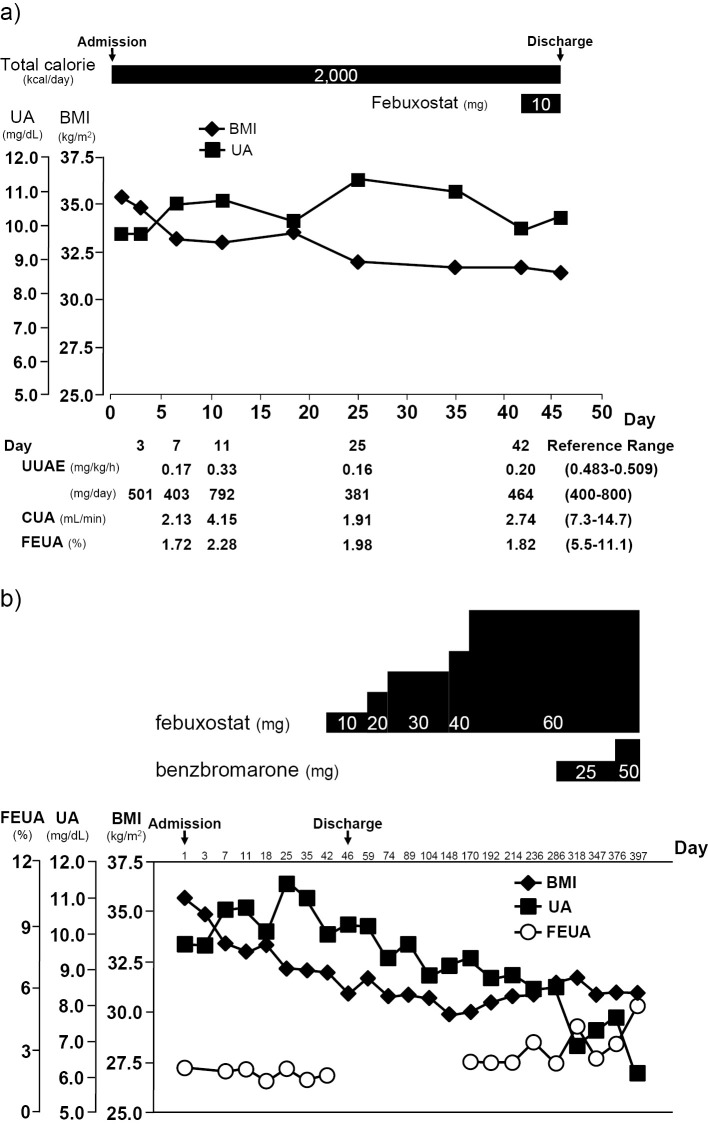
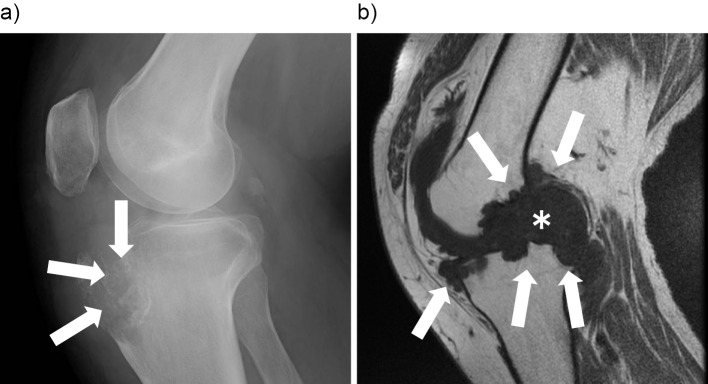
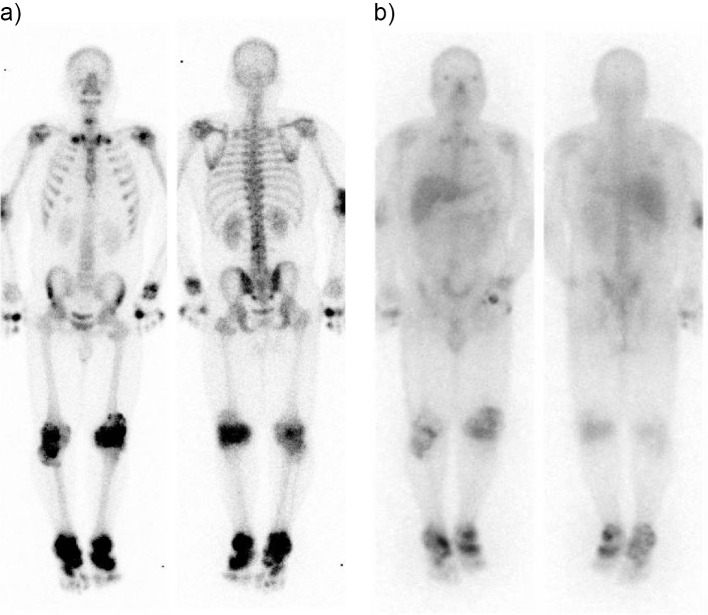
A 27 year-old severely obese man (BMI, 35.1) had hyperuricemia and multiple gouty tophi with bone erosion and destruction, resulting in gait disturbance for 6 years after the early onset of gout at 21 years of age. His hyperuricemia was associated with hyperinsulinemia in obesity and a genetic variant of the ABCG2 gene. In addition, multiple gouty tophi with bone erosion and destruction might have been caused by hypoadiponectinemia and the elevation of the patient' s pro-inflammatory cytokine (IL-1β) level with the accumulation of visceral fat. In this case, bone and Ga-67 scintigraphy were useful for detecting the location and magnitude of gouty tophi.
一名27岁的严重肥胖男子(体重指数,35.1)患有高尿酸血症和多处痛风石,伴有骨质侵蚀和破坏,自21岁痛风初发后6年导致步态障碍。他的高尿酸血症与肥胖中的高胰岛素血症以及ABCG2基因的一个遗传变异有关。此外,多处伴有骨质侵蚀和破坏的痛风石可能是由低脂联素血症以及患者促炎细胞因子(IL-1β)水平随内脏脂肪堆积而升高所致。在该病例中,骨显像和Ga-67闪烁扫描对于检测痛风石的位置和大小很有用。