Department of Oncology, University of Cambridge, Cambridge.
NIHR Cambridge Biomedical Research Centre, Cambridge.
Ann Oncol. 2017 Aug 1;28(8):1817-1824. doi: 10.1093/annonc/mdx173.
The ARTemis trial previously reported that addition of neoadjuvant bevacizumab (Bev) to docetaxel (D) followed by fluorouracil, epirubicin and cyclophosphamide (D-FEC) in HER2 negative breast cancer improved the pathological complete response (pCR) rate. We present disease-free survival (DFS) and overall survival (OS) with central pathology review.
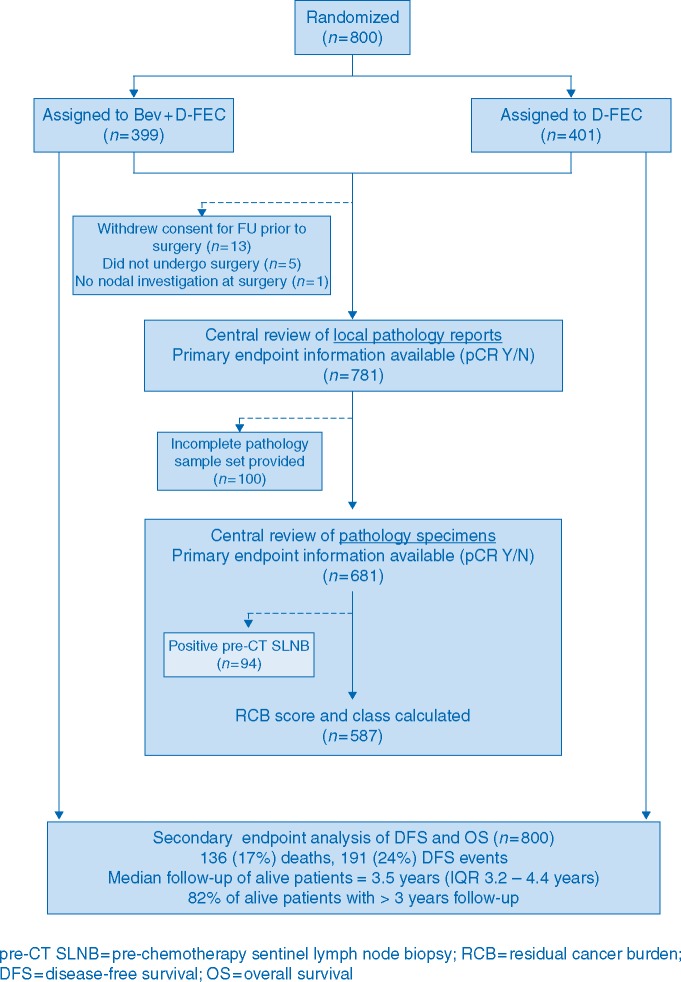
Patients were randomized to 3 cycles of D followed by 3 cycles of FEC (D-FEC), ±4 cycles of Bev (Bev + D-FEC). DFS and OS were analyzed by treatment and by central pathology reviewed pCR and Residual Cancer Burden (RCB) class.
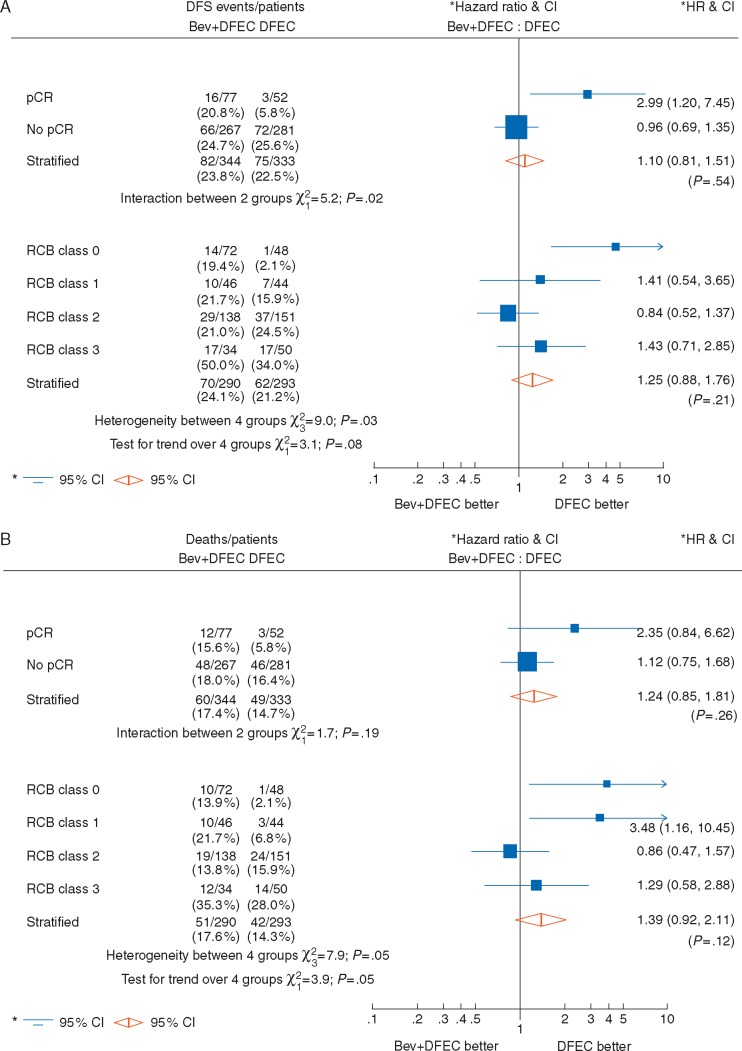
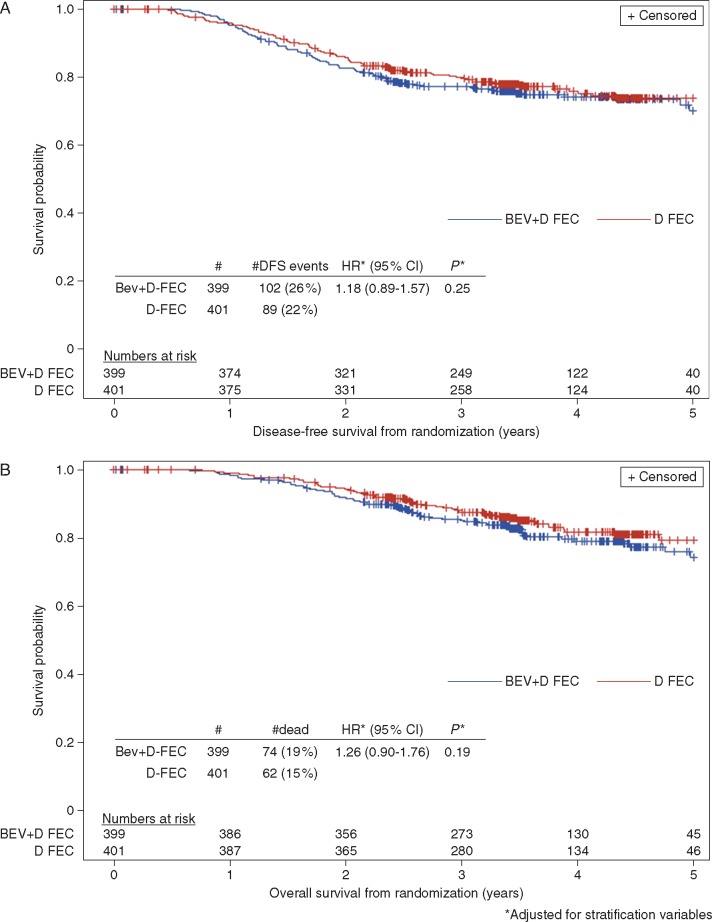
A total of 800 patients were randomized [median follow-up 3.5 years (IQR 3.2-4.4)]. DFS and OS were similar across treatment arms [DFS hazard ratio (HR)=1.18 (95% CI 0.89-1.57), P = 0.25; OS HR = 1.26 (95% CI 0.90-1.76), P = 0.19). Both local pathology report review and central histopathology review confirmed a significant improvement in DFS and OS for patients who achieved a pCR [DFS HR = 0.38 (95% CI 0.23-0.63), P < 0.001; OS HR = 0.43 (95% CI 0.24-0.75), P = 0.003]. However, significant heterogeneity was observed (P = 0.02); larger improvements in DFS were obtained with a pCR achieved with D-FEC than a pCR achieved with Bev + D-FEC. As RCB class increased, significantly worse DFS and OS was observed (P for trend <0.0001), which effect was most marked in the ER negative group.
The addition of short course neoadjuvant Bev to standard chemotherapy did not demonstrate a DFS or OS benefit. Achieving a pCR with D-FEC is associated with improved DFS and OS but not when pCR is achieved with Bev + D-FEC. At the present time therefore, Bev is not recommended in early breast cancer.
CLINICALTRIALS.GOV NUMBER: NCT01093235.
ARTemis 试验先前报道,在 HER2 阴性乳腺癌中,将新辅助贝伐单抗(Bev)加入多西他赛(D),然后加入氟尿嘧啶、表柔比星和环磷酰胺(D-FEC),可提高病理完全缓解(pCR)率。我们报告了中心病理评估的无病生存(DFS)和总生存(OS)。
患者被随机分配接受 3 个周期的 D 治疗,然后接受 3 个周期的 FEC(D-FEC),±4 个周期的 Bev(Bev+D-FEC)。DFS 和 OS 通过治疗和中心病理评估的 pCR 和残留肿瘤负担(RCB)分类进行分析。
共 800 例患者随机分组[中位随访 3.5 年(IQR 3.2-4.4)]。DFS 和 OS 在治疗组之间无差异[DFS 风险比(HR)=1.18(95%CI 0.89-1.57),P=0.25;OS HR=1.26(95%CI 0.90-1.76),P=0.19]。局部病理报告评估和中心组织病理学评估均证实,pCR 患者的 DFS 和 OS 显著改善[DFS HR=0.38(95%CI 0.23-0.63),P<0.001;OS HR=0.43(95%CI 0.24-0.75),P=0.003]。然而,观察到显著的异质性(P=0.02);与 Bev+D-FEC 相比,D-FEC 实现的 pCR 可获得更大的 DFS 改善。随着 RCB 级别的增加,DFS 和 OS 明显变差(趋势 P<0.0001),在 ER 阴性组中这种影响最为显著。
短期新辅助贝伐单抗联合标准化疗并未显示出 DFS 或 OS 获益。与 Bev+D-FEC 相比,D-FEC 实现的 pCR 与改善的 DFS 和 OS 相关,但 Bev+D-FEC 实现的 pCR 则不然。目前,贝伐单抗不推荐用于早期乳腺癌。
NCT01093235。