Manion Maura, Hullsiek Katherine Huppler, Wilson Eleanor M P, Rhame Frank, Kojic Erna, Gibson David, Hammer John, Patel Pragna, Brooks John T, Baker Jason V, Sereti Irini
National Institute of Allergy and Infectious Disease, National Institutes of Health, Bethesda, Maryland, United States of America.
Division of Biostatistics, University of Minnesota, Minneapolis, Minnesota, United States of America.
PLoS One. 2017 May 2;12(5):e0175517. doi: 10.1371/journal.pone.0175517. eCollection 2017.
Immune activation plays a key role in HIV pathogenesis. Markers of inflammation have been associated with vitamin D deficiency in the general population. Studies have also demonstrated associations of vitamin D deficiency with increased risk of HIV progression and death. The relationship between persistent inflammation and immune activation during chronic HIV infection and vitamin D deficiency remains unclear.
Cryopreserved specimens were analyzed from 663 participants at the time of enrollment from the Study to Understand the Natural History of HIV/AIDS in the Era of Effective Therapy (SUN Study) from 2004 to 2006. Biomarkers of inflammation, atherosclerosis, and coagulation were measured using enzyme-linked immunosorbent assays (ELISAs) and electrochemiluminescence. 25(OH)D, the stable precursor form of vitamin D, was measured using a radioimmunoassay with levels defined as: normal (≥30ng/mL), insufficient (20-29 ng/mL) and deficient (<20 ng/mL). Monocyte phenotypes were assessed by flow cytometry. Linear and logistic regression models were used to determine statistical associations between biomarkers and vitamin D deficiency.
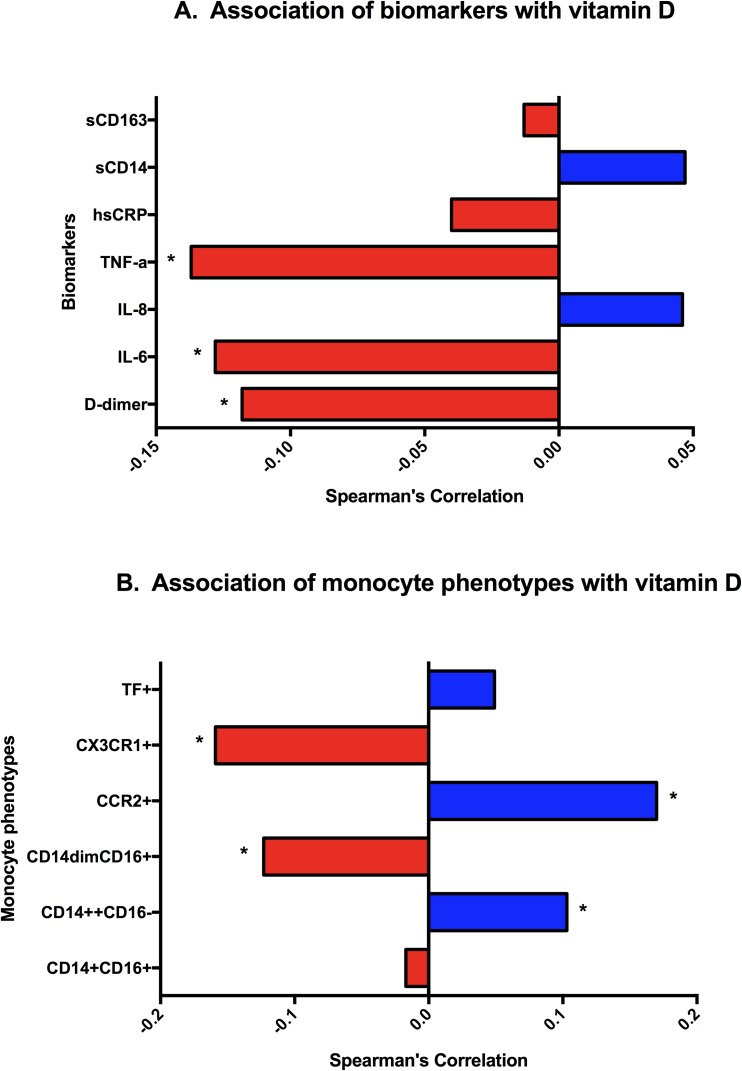
25(OH)D levels were deficient in 251 (38%) participants, insufficient in 222 (34%), and normal in 190 (29%). Patients with vitamin D deficiency, when compared to those with insufficient or normal vitamin D levels, had increased levels of IL-6 (23%; p<0.01), TNF-α (21%, p = 0.03), D-dimer (24%, p = 0.01), higher proportions of CD14dimCD16+ (22%, p<0.01) and CX3CR1+ monocytes (48%; p<0.001) and decreased frequency of CCR2+ monocytes (-3.4%, p<0.001). In fully adjusted models, vitamin D associations with abnormal biomarker levels persisted for IL-6 levels and CX3CR1+ and CCR2+ phenotypes.
Vitamin D deficiency is associated with greater inflammation and activated monocyte phenotypes. The role of vitamin D deficiency in persistent immune activation and associated complications during chronic HIV disease should be further evaluated as a possible target for intervention.
免疫激活在HIV发病机制中起关键作用。在普通人群中,炎症标志物与维生素D缺乏有关。研究还表明维生素D缺乏与HIV进展和死亡风险增加有关。慢性HIV感染期间持续炎症与免疫激活以及维生素D缺乏之间的关系仍不清楚。
对2004年至2006年“了解有效治疗时代HIV/AIDS自然史研究”(SUN研究)入组时663名参与者的冷冻保存标本进行分析。使用酶联免疫吸附测定(ELISA)和电化学发光法测量炎症、动脉粥样硬化和凝血的生物标志物。使用放射免疫测定法测量维生素D的稳定前体形式25(OH)D,其水平定义为:正常(≥30ng/mL)、不足(20 - 29 ng/mL)和缺乏(<20 ng/mL)。通过流式细胞术评估单核细胞表型。使用线性和逻辑回归模型确定生物标志物与维生素D缺乏之间的统计关联。
251名(38%)参与者的25(OH)D水平缺乏,222名(34%)不足,190名(29%)正常。与维生素D水平不足或正常者相比,维生素D缺乏患者的IL-6水平升高(23%;p<0.01)、TNF-α升高(21%,p = 0.03)、D-二聚体升高(24%,p = 0.01),CD14dimCD16+单核细胞比例更高(22%,p<0.01)和CX3CR1+单核细胞比例更高(48%;p<0.001),而CCR2+单核细胞频率降低(-3.4%,p<0.001)。在完全调整模型中,维生素D与异常生物标志物水平的关联在IL-6水平以及CX3CR1+和CCR2+表型方面仍然存在。
维生素D缺乏与更严重的炎症和活化的单核细胞表型有关。维生素D缺乏在慢性HIV疾病期间持续免疫激活及相关并发症中的作用应作为可能的干预靶点进一步评估。