Briere Tina Marie, McAleer Mary Frances, Levy Lawrence B, Yang James N
Departments of Radiation Physics, UT MD Anderson Cancer Center, 1400 Pressler St., Unit #1420, Houston, TX, 77030, USA.
Departments of Radiation Oncology, UT MD Anderson Cancer Center, Houston, TX, USA.
Radiat Oncol. 2017 May 2;12(1):79. doi: 10.1186/s13014-017-0810-3.
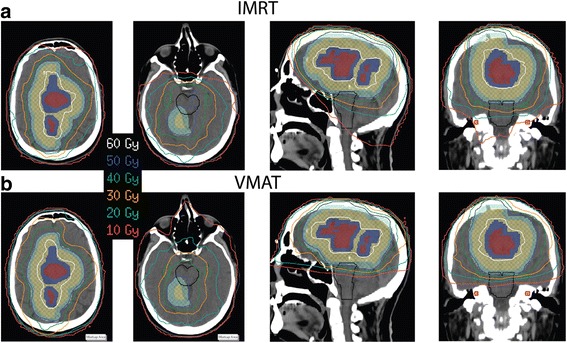
Patients with glioblastoma multiforme (GBM) require radiotherapy as part of definitive management. Our institution has adopted the use of volumetric arc therapy (VMAT) due to superior sparing of the adjacent organs at risk (OARs) compared to intensity modulated radiation therapy (IMRT). Here we report our clinical experience by analyzing target coverage and sparing of OARs for 90 clinical treatment plans.
VMAT and IMRT patient cohorts comprising 45 patients each were included in this study. For all patients, the planning target volume (PTV) received 50 Gy in 30 fractions, and the simultaneous integrated boost PTV received 60 Gy. The characteristics of the two patient cohorts were examined for similarity. The doses to target volumes and OARs, including brain, brainstem, hippocampi, optic nerves, eyes, and cochleae were then compared using statistical analysis. Target coverage and normal tissue sparing for six patients with both clinical IMRT and VMAT plans were analyzed.
PTV coverage of at least 95% was achieved for all plans, and the median mean dose to the boost PTV differed by only 0.1 Gy between the IMRT and VMAT plans. Superior sparing of the brainstem was found with VMAT, with a median difference in mean dose being 9.4 Gy. The ipsilateral cochlear mean dose was lower by 19.7 Gy, and the contralateral cochlea was lower by 9.5 Gy. The total treatment time was reduced by 5 min. The difference in the ipsilateral hippocampal D was 12 Gy, though this is not statistically significant (P = 0.03).
VMAT for GBM patients can provide similar target coverage, superior sparing of the brainstem and cochleae, and be delivered in a shorter period of time compared with IMRT. The shorter treatment time may improve clinical efficiency and the quality of the treatment experience. Based on institutional clinical experience, use of VMAT for the treatment of GBMs appears to offer no inferiority in comparison to IMRT and may offer distinct advantages, especially for patients who may require re-irradiation.
多形性胶质母细胞瘤(GBM)患者需要放疗作为确定性治疗的一部分。与调强放射治疗(IMRT)相比,由于能更好地保护相邻危及器官(OARs),我们机构已采用容积弧形调强放疗(VMAT)。在此,我们通过分析90个临床治疗计划的靶区覆盖情况和OARs的保护情况来报告我们的临床经验。
本研究纳入了各45例患者的VMAT和IMRT患者队列。所有患者的计划靶区(PTV)接受30次分割共50 Gy的照射,同步整合加量PTV接受60 Gy的照射。检查两个患者队列的特征是否相似。然后使用统计分析比较靶区和OARs(包括脑、脑干、海马、视神经、眼睛和耳蜗)的剂量。分析了6例同时有IMRT和VMAT临床计划患者的靶区覆盖和正常组织保护情况。
所有计划均实现了至少95%的PTV覆盖,IMRT和VMAT计划中加量PTV的中位平均剂量仅相差0.1 Gy。发现VMAT对脑干的保护更好,平均剂量的中位差异为9.4 Gy。同侧耳蜗平均剂量降低19.7 Gy,对侧耳蜗降低9.5 Gy。总治疗时间减少了5分钟。同侧海马D的差异为12 Gy,尽管这无统计学意义(P = 0.03)。
与IMRT相比,GBM患者的VMAT可提供相似的靶区覆盖,更好地保护脑干和耳蜗,且治疗时间更短。较短的治疗时间可能会提高临床效率和治疗体验质量。基于机构临床经验,VMAT治疗GBM与IMRT相比似乎并无劣势,且可能具有明显优势,尤其是对于可能需要再次放疗的患者。