Wai Elaine S, Lesperance Mary, Lu Linghong, Alexander Cheryl S, Truong Pauline T
Radiation Oncology, University of British Columbia, BC Cancer Agency.
Statistics, University of Victoria.
Cureus. 2017 Mar 31;9(3):e1128. doi: 10.7759/cureus.1128.
Management of ductal carcinoma in situ (DCIS) remains controversial. This study examined long-term outcomes in a population-based cohort of patients with pure DCIS treated with breast-conserving surgery (BCS) alone, BCS + radiotherapy (RT), and mastectomy. Outcomes were compared between patients referred versus not referred for oncologic assessment after definitive surgery.
Subjects were 2575 women diagnosed between 1985 and 1999. Data from several electronic databases were linked and analyzed. Outcomes were invasive local recurrence-free survival (ILRFS), mastectomy-free survival (MFS), breast cancer-specific survival (BCSS), and overall survival (OS).
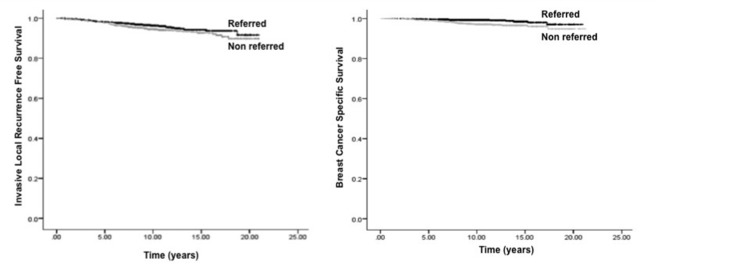
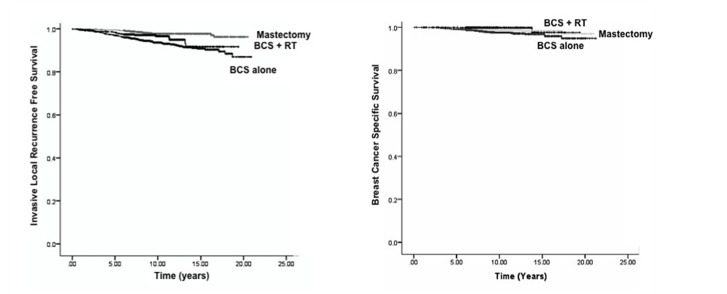
Median follow-up time was 9.8 years. Overall, 56% (n = 1448) of subjects were referred to a cancer centre. Factors associated with non-referral were older age, comorbidities, and travel distance. Ten-year MFS, BCSS, and OS were higher among referred patients (all p ≤ 0.001). In cohorts treated with BCS alone (n = 1314) vs. BCS + RT (n = 510) vs. mastectomy (n = 751), 10-year ILRFS were 93.7% vs. 96.6% vs. 97.7%, (p < 0.001) and BCSS were 97.6% vs. 99.8% vs. 98.6%, (p = 0.01). Corresponding rates of ipsilateral invasive breast relapse at 10 years were 6.3% after BCS alone, 3.4% after BCS + RT, and 2.3% after mastectomy (p < 0.001). On multivariable analysis, factors associated with improved ILRFS were older age at diagnosis, low comorbidity score, absence of comedo histology, mastectomy, and post-BCS RT.
Patients with DCIS referred for oncologic assessment were more likely to undergo post-BCS RT, resulting in lower mastectomy and higher survival rates compared to non-referred patients. Patients with significant comorbidities were less likely to be referred and experienced lower ILRFS and BCSS. Referral for multidisciplinary oncologic assessment after surgery is warranted to individualize management and optimize outcomes for patients with DCIS.
导管原位癌(DCIS)的治疗仍存在争议。本研究调查了一组以人群为基础的单纯接受保乳手术(BCS)、BCS+放疗(RT)和乳房切除术的纯DCIS患者的长期预后。比较了确诊手术后转诊和未转诊接受肿瘤学评估的患者的预后。
研究对象为1985年至1999年间确诊的2575名女性。对来自多个电子数据库的数据进行了关联和分析。预后指标为无局部浸润性复发生存率(ILRFS)、无乳房切除生存率(MFS)、乳腺癌特异性生存率(BCSS)和总生存率(OS)。
中位随访时间为9.8年。总体而言,56%(n=1448)的研究对象被转诊至癌症中心。与未转诊相关的因素包括年龄较大、合并症和出行距离。转诊患者的10年MFS、BCSS和OS更高(所有p≤0.001)。在单纯接受BCS治疗的队列(n=1314)、BCS+RT治疗的队列(n=510)和乳房切除术治疗的队列(n=751)中,10年ILRFS分别为93.7%、96.6%和97.7%,(p<0.001),BCSS分别为97.6%、99.8%和98.6%,(p=0.01)。10年时同侧浸润性乳腺癌复发率在单纯BCS后为6.3%,BCS+RT后为3.4%,乳房切除术后为2.3%(p<0.001)。多变量分析显示,与ILRFS改善相关的因素包括诊断时年龄较大、合并症评分低、无粉刺样组织学、乳房切除术和BCS后放疗。
转诊接受肿瘤学评估的DCIS患者更有可能接受BCS后放疗,与未转诊患者相比,乳房切除术率更低,生存率更高。合并症严重的患者被转诊的可能性较小,ILRFS和BCSS较低。手术后转诊进行多学科肿瘤学评估对于DCIS患者的个体化治疗和优化预后是必要的。