Ostermann Marlies, Hall Anna, Crichton Siobhan
Department of Critical Care, King's College London, Guy's & St Thomas' NHS Foundation Trust, Westminster Bridge Road SE1 7 EH, London, UK.
Department of Critical Care, Guy's & St Thomas' NHS Foundation Trust, Westminster Bridge Road, London, SE1 7EH, UK.
BMC Nephrol. 2017 May 3;18(1):151. doi: 10.1186/s12882-017-0568-8.
The aim was to investigate whether mean perfusion pressure (MPP) calculated as the difference between mean arterial pressure (MAP) and central venous pressure (CVP) was associated with risk of progression from AKI I to AKI III in critically ill patients.
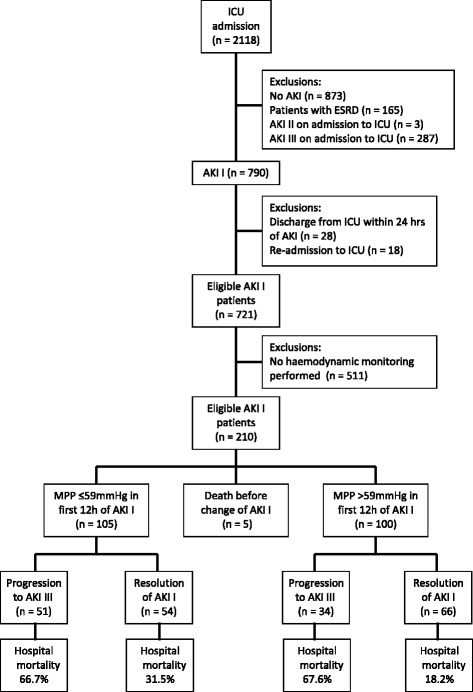
Retrospective analysis of adult patients admitted to a multi-disciplinary adult intensive care unit (ICU) between July 2007 and June 2009 who developed AKI I and in whom advanced haemodynamic monitoring was initiated within 12 h of diagnosis of AKI I. We compared patients with a MPP above and below the median value in the first 12 h of diagnosis of AKI. Multivariable logistic regression analyses were performed to identify independent risk factors for progression to AKI III, to explore the impact of MAP and CVP separately, and to investigate the impact of MPP in pre-defined sub-groups.
Among 2118 ICU patients, 790 patients (37%) developed AKI I of whom 205 underwent advanced haemodynamic monitoring within 12 h of AKI stage I. Their median MPP was 59 mmHg. AKI I patients with a MPP ≤59 mmHg had a significantly higher risk of progressing to AKI stage III (48.6% versus 34%, respectively; p = 0.0034). This association was stronger in patients with ischemic heart disease, congestive cardiac failure or without pre-existing hypertension and in patients with a MAP <65 mmHg for >1 h. As individual components, a raised CVP was independently associated with progression to AKI stage III but MAP alone was not an independent risk factor for AKI progression.
MPP <60 mmHg was independently associated with AKI progression. CVP was the key component of MPP.
目的是研究以平均动脉压(MAP)与中心静脉压(CVP)之差计算所得的平均灌注压(MPP)是否与危重症患者急性肾损伤(AKI)I期进展至AKI III期的风险相关。
对2007年7月至2009年6月入住多学科成人重症监护病房(ICU)且发生AKI I期、在诊断AKI I期后12小时内开始进行高级血流动力学监测的成年患者进行回顾性分析。我们比较了在诊断AKI的前12小时内MPP高于和低于中位数的患者。进行多变量逻辑回归分析以确定进展至AKI III期的独立危险因素,分别探讨MAP和CVP的影响,并研究MPP在预定义亚组中的影响。
在2118例ICU患者中,790例(37%)发生AKI I期,其中205例在AKI I期12小时内接受了高级血流动力学监测。他们的MPP中位数为59 mmHg。MPP≤59 mmHg的AKI I期患者进展至AKI III期的风险显著更高(分别为48.6%和34%;p = 0.0034)。这种关联在患有缺血性心脏病、充血性心力衰竭或无既往高血压的患者以及MAP<65 mmHg超过1小时的患者中更强。作为单独的组成部分,CVP升高与进展至AKI III期独立相关,但单独的MAP不是AKI进展的独立危险因素。
MPP<60 mmHg与AKI进展独立相关。CVP是MPP的关键组成部分。