a Intensive Care Unit , Dr. Kenessey Albert Hospital , Balassagyarmat , Hungary.
b Faculty of Health Sciences, Department of Clinical Studies , Semmelweis University , Budapest , Hungary.
Ren Fail. 2019 Nov;41(1):150-158. doi: 10.1080/0886022X.2019.1587467.
The incidence of postoperative acute kidney injury (AKI) is predominantly determined by renal hemodynamics. Beside arterial blood pressure, the role of factors causing a deterioration of venous congestion (intraabdominal pressure, central venous pressure, mechanical ventilation) has emerged. The value of combined hemodynamic, respiratory and intra-abdominal pressure (IAP) monitoring in predicting postoperative acute kidney injury has received only limited exploration to date.
Data were collected for adult patients admitted after major abdominal surgery at nine Hungarian ICUs. Hemodynamic parameters were compared in AKI vs. no-AKI patients at the time of admission and 48 h thereafter. Regarding ventilatory support, we tested mean airway pressures (Pmean). Effective renal perfusion pressure (RPP) was calculated as MAP-(IAP + CVP + Pmean). The Mann-Whitney U and the chi-square tests were carried out for statistical analysis with forward stepwise logistic regression for AKI as a dependent outcome.
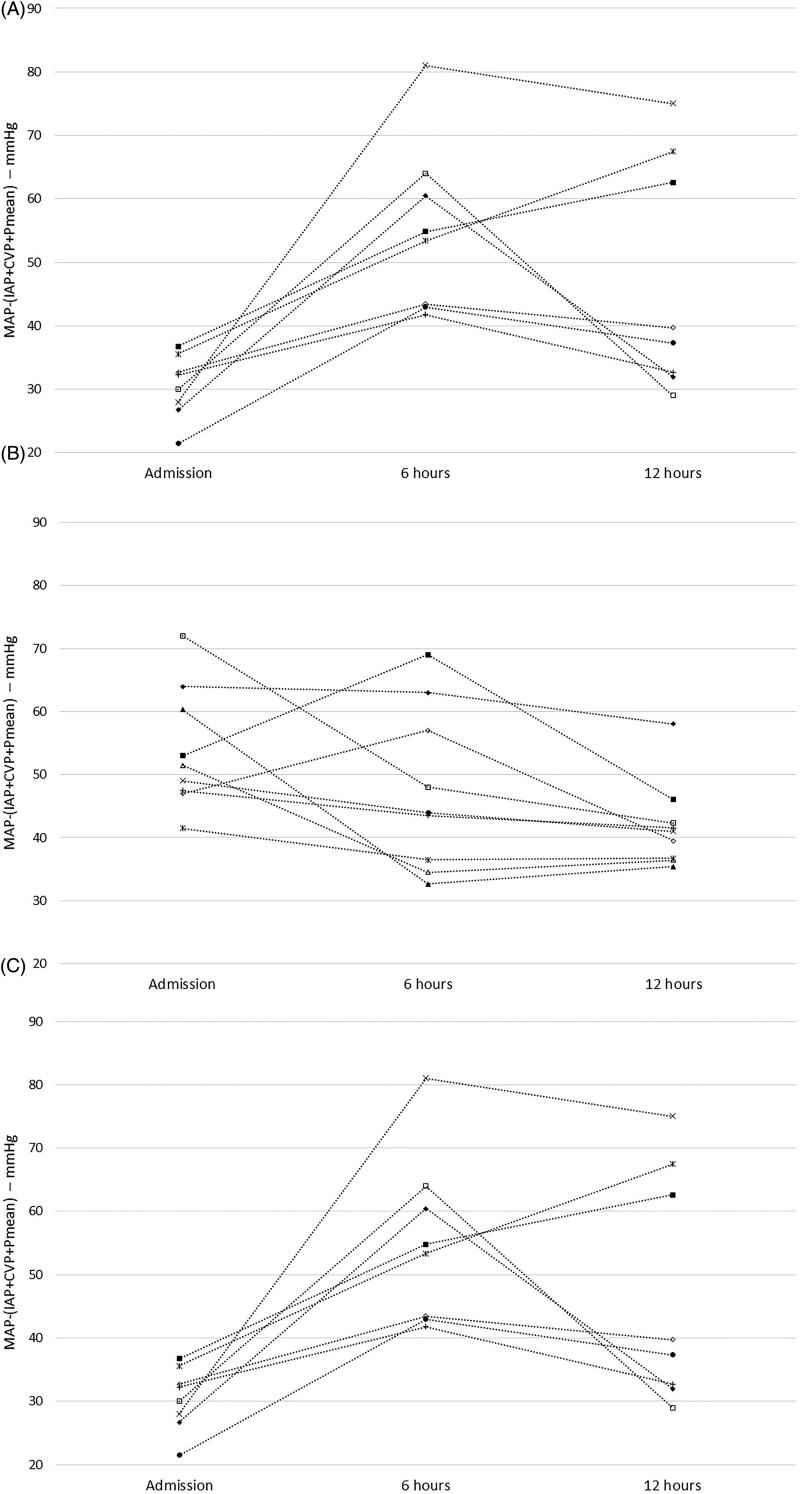
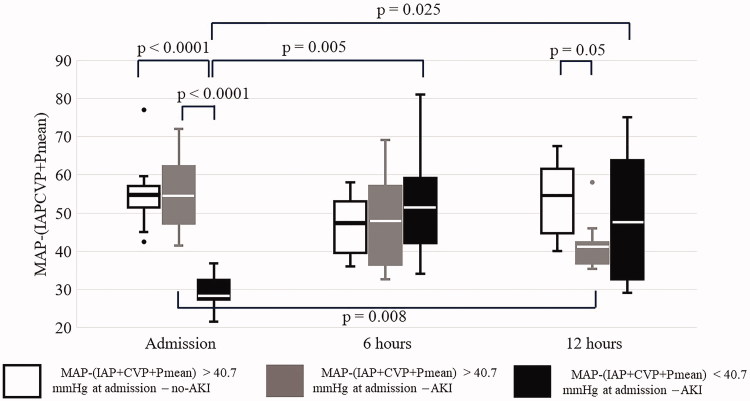
A total of 84 patients (34 ventilated) were enrolled in our multicenter observational study. The median values of MAP were above 70 mmHg, IAP not higher than 12 mmHg and CVP not higher than 8 mmHg at all time-points. When we combined those parameters, even those belonging to the 'normal' range with Pmean, we found significant differences between no-AKI and AKI groups only at 12 h after ICU admission (median and IQR: 57 (42-64) vs. 40 (36-52); p < .05). Below it's median (40.7 mmHg) on admission, AKI developed in all patients. If above 40.7 mmHg on admission, they were protected against AKI, but only if it did not decrease within the first 12 h.
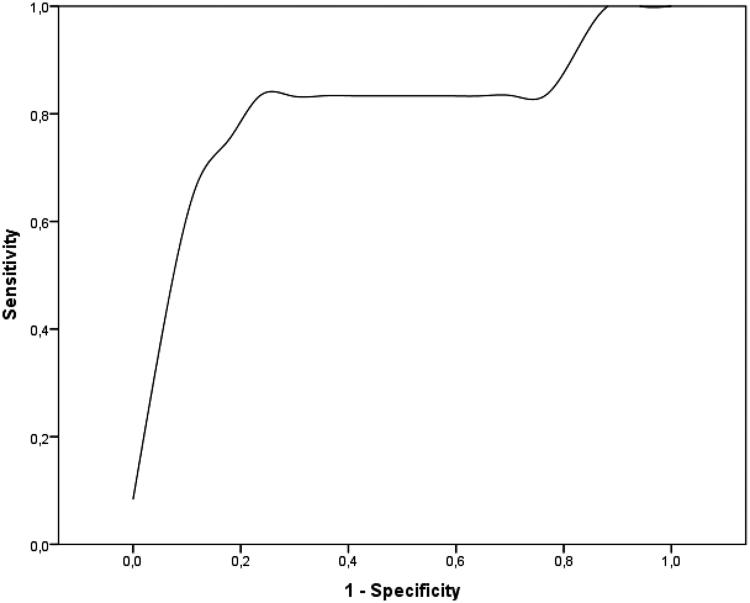
Calculated effective RPP with the novel formula MAP-(IAP + CVP + Pmean) may predict the onset of AKI in the surgical ICU with a great sensitivity and specificity. Maintaining effective RPP appears important not only at ICU admission but during the next 12 h, as well. Additional, larger studies are needed to explore therapeutic interventions targeting this parameter.
术后急性肾损伤(AKI)的发生率主要取决于肾脏的血液动力学。除了动脉血压外,导致静脉充血恶化的因素(腹内压、中心静脉压、机械通气)的作用也已经显现出来。目前,联合血液动力学、呼吸和腹内压(IAP)监测在预测术后急性肾损伤方面的价值仅受到有限的探索。
本研究在匈牙利的 9 家 ICU 收集了接受大型腹部手术后的成年患者的数据。在入院时和入院后 48 小时,比较 AKI 患者和非 AKI 患者的血液动力学参数。在通气支持方面,我们测试了平均气道压力(Pmean)。有效肾灌注压(RPP)的计算方法为 MAP-(IAP+CVP+Pmean)。采用曼-惠特尼 U 检验和卡方检验进行统计学分析,采用向前逐步逻辑回归分析 AKI 作为因变量。
我们的多中心观察性研究共纳入 84 例患者(34 例机械通气)。在所有时间点,MAP 的中位数均高于 70mmHg,IAP 不高于 12mmHg,CVP 不高于 8mmHg。当我们将这些参数结合起来时,即使是那些与 Pmean 一起属于“正常”范围的参数,我们也仅在 ICU 入院后 12 小时发现 AKI 组和非 AKI 组之间存在显著差异(中位数和四分位距:57(42-64)与 40(36-52);p<.05)。在入院时,其中位数(40.7mmHg)以下,所有患者均发生 AKI。如果入院时大于 40.7mmHg,他们就可以免受 AKI 的影响,但只有在入院后 12 小时内没有下降。
用新公式 MAP-(IAP+CVP+Pmean)计算的有效 RPP 可能具有很高的灵敏度和特异性,可以预测外科 ICU 中 AKI 的发生。维持有效 RPP 不仅在 ICU 入院时很重要,在接下来的 12 小时内也很重要。需要进行更多更大的研究来探索针对这一参数的治疗干预措施。