Wilson Henrietta, Gammon David, Routledge Tom, Harrison-Phipps Karen
Department of Thoracic Surgery, Guy's Hospital, Great Maze Pond, London, SE1 9RT, UK.
Ann Thorac Med. 2017 Apr-Jun;12(2):83-87. doi: 10.4103/atm.ATM_385_16.
Surgery remains the gold standard for patients with resectable nonsmall cell lung cancer. Current guidance identifies patients with poor pulmonary reserve to fall within a high-risk cohort. The aim of this study was to determine the clinical and quality of life outcomes of anatomical lung resection in patients deemed high risk based on pulmonary function measurements.
A retrospective review of patients undergoing anatomical lung resection for nonsmall cell lung cancer between January 2013 and January 2015 was performed. All patients with limited pulmonary reserve defined as predicted postoperative forced expiratory volume in 1 s or transfer factor of the lung for carbon monoxide of <40% were included in the study. Postoperative complications, admission to the Intensive Care Unit, length of stay, and 30-day in-hospital mortality were recorded. The European Organization for Research and Treatment of Cancer quality of life questionnaire lung cancer 13 questionnaire was used to assess quality of life outcomes.
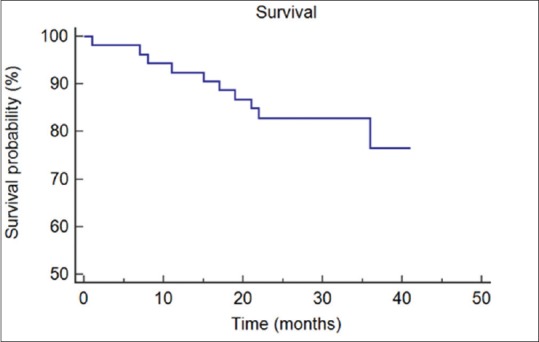
Fifty-three patients met the inclusion criteria. There was no in-hospital mortality, and 30-day mortality was 1.8%. No complications were seen in 64% ( = 34), minor complications occurred in 26% ( = 14), while 9% had a major complication ( = 5). Quality of life outcomes were above the reference results for patients with early stage lung cancer.
Anatomical lung resection can be performed safely in selected high-risk patients based on pulmonary function without significant increase in morbidity or mortality and with acceptable quality of life outcomes. Given that complications following lung resection are multifactorial, fitness for surgery should be thoroughly assessed in all patients with resectable disease within a multidisciplinary setting. High operative risk by pulmonary function tests alone should not preclude surgical resection.
手术仍然是可切除非小细胞肺癌患者的金标准。当前指南将肺储备功能差的患者归为高风险队列。本研究的目的是确定基于肺功能测量被视为高风险的患者进行肺叶切除术后的临床和生活质量结果。
对2013年1月至2015年1月期间因非小细胞肺癌接受肺叶切除的患者进行回顾性研究。所有肺储备功能受限(定义为术后预测1秒用力呼气量或肺一氧化碳转运因子<40%)的患者均纳入研究。记录术后并发症、入住重症监护病房情况、住院时间和30天院内死亡率。使用欧洲癌症研究与治疗组织肺癌生活质量问卷13进行生活质量结果评估。
53例患者符合纳入标准。无院内死亡,30天死亡率为1.8%。64%(n = 34)的患者未出现并发症,26%(n = 14)出现轻微并发症,9%(n = 5)出现严重并发症。生活质量结果高于早期肺癌患者的参考结果。
对于基于肺功能选择的高风险患者,可安全地进行肺叶切除,发病率和死亡率无显著增加,生活质量结果可接受。鉴于肺切除术后并发症是多因素的,应在多学科环境中对所有可切除疾病患者进行全面的手术适应性评估。仅通过肺功能测试判断的高手术风险不应排除手术切除。