Alcoba Gabriel, Keitel Kristina, Maspoli Veronica, Lacroix Laurence, Manzano Sergio, Gehri Mario, Tabin René, Gervaix Alain, Galetto-Lacour Annick
Division of Pediatric Emergency Medicine, Department of Child and Adolescent Medicine, Geneva University Hospitals and University of Geneva, Geneva, Switzerland.
Division of Tropical and Humanitarian Medicine, Geneva University Hospitals (Hôpitaux Universitaires de Genève, HUG), Rue Gabrielle-Perret-Gentil 4, CH-1211, Genève 14, Switzerland.
Eur J Pediatr. 2017 Jun;176(6):815-824. doi: 10.1007/s00431-017-2913-0. Epub 2017 May 4.
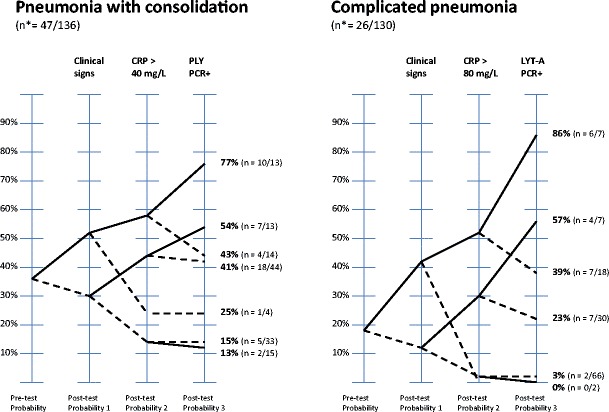
Recommendations for the management of community-acquired pneumonia (CAP) advocate that, in the absence of the clinical and laboratory findings typical of bacterial CAP, antibiotics are not required. However, the true value of the clinical and laboratory predictors of pediatric CAP still needs to be assessed. This prospective cohort study in three emergency departments enrolled 142 children with radiological pneumonia. Pneumonia with lung consolidation was the primary endpoint; complicated pneumonia (bacteremia, empyema, or pleural effusion) was the secondary endpoint. We showed that three clinical signs (unilateral hypoventilation, grunting, and absence of wheezing), elevated procalcitonin (PCT), C-reactive protein (CRP), negative nasopharyngeal viral PCR, or positive blood pneumococcal PCR (P-PCR) were significantly associated with both pneumonia with consolidation and complicated pneumonia. Children with negative clinical signs and low CRP values had a low probability of having pneumonia with consolidation (13%) or complicated pneumonia (6%). Associating the three clinical signs, CRP >80 mg/L and a positive P-PCR ruled in the diagnosis of complicated pneumonia with a positive predictive value of 75%.
A model incorporating clinical signs and laboratory markers can effectively assess the risk of having pneumonia. Children with negative clinical signs and low CRP are at a low risk of having pneumonia. For children with positive clinical signs and high CRP, a positive blood pneumococcal PCR can more accurately confirm the diagnosis of pneumonia. What is Known: • Distinguishing between bacterial and viral pneumonia in children is challenging. • Reducing the inappropriate use of antibiotics is a priority. What is New: • Children with negative clinical signs and low C-reactive protein (CRP) values have a low probability of having pneumonia. • Children with high CRP values can be tested using a pneumococcal PCR to rule in the diagnosis of pneumonia with a high positive predictive value.
社区获得性肺炎(CAP)管理指南建议,在缺乏典型细菌性CAP的临床和实验室检查结果时,无需使用抗生素。然而,小儿CAP临床和实验室预测指标的真正价值仍有待评估。这项前瞻性队列研究在三个急诊科纳入了142例患有放射性肺炎的儿童。以肺部实变的肺炎为主要终点;复杂性肺炎(菌血症、脓胸或胸腔积液)为次要终点。我们发现,三个临床体征(单侧通气不足、呻吟和无喘息)、降钙素原(PCT)升高、C反应蛋白(CRP)升高、鼻咽部病毒PCR阴性或血肺炎球菌PCR(P-PCR)阳性与肺部实变的肺炎和复杂性肺炎均显著相关。临床体征阴性且CRP值低的儿童发生肺部实变肺炎(13%)或复杂性肺炎(6%)的概率较低。将三个临床体征、CRP>80mg/L和P-PCR阳性相结合可确诊复杂性肺炎,阳性预测值为75%。
结合临床体征和实验室指标的模型可有效评估患肺炎的风险。临床体征阴性且CRP低的儿童患肺炎的风险较低。对于临床体征阳性且CRP高的儿童,血肺炎球菌PCR阳性可更准确地确诊肺炎。已知信息:• 区分儿童细菌性和病毒性肺炎具有挑战性。• 减少抗生素的不恰当使用是一项优先任务。新发现:• 临床体征阴性且C反应蛋白(CRP)值低的儿童患肺炎的概率较低。• CRP值高的儿童可通过肺炎球菌PCR检测来确诊肺炎且具有较高的阳性预测值。