Dagnino Giulio, Georgilas Ioannis, Morad Samir, Gibbons Peter, Tarassoli Payam, Atkins Roger, Dogramadzi Sanja
Bristol Robotics Laboratory, University of the West of England, Coldharbour Lane, BS161QY, Bristol, UK.
Aston University, B47ET, Birmingham, UK.
Int J Comput Assist Radiol Surg. 2017 Aug;12(8):1383-1397. doi: 10.1007/s11548-017-1602-9. Epub 2017 May 4.
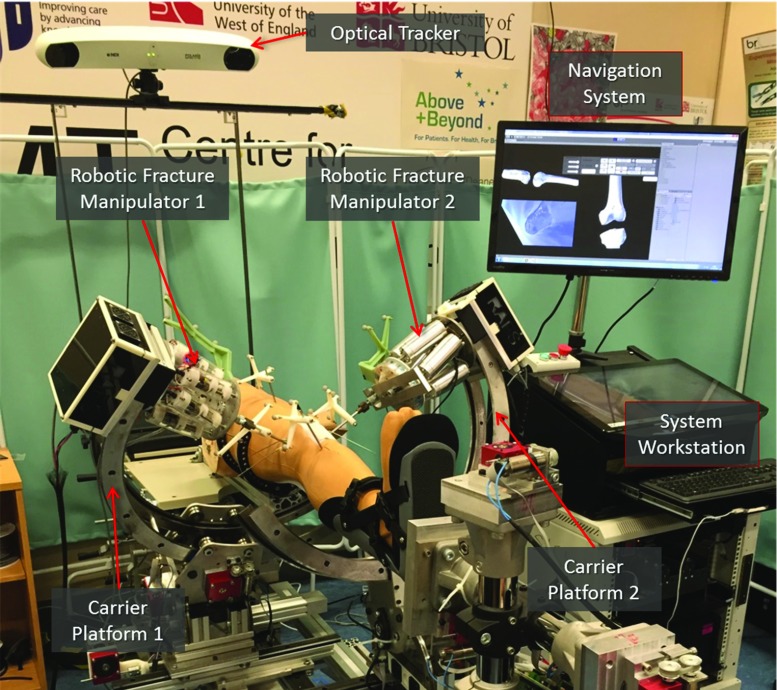
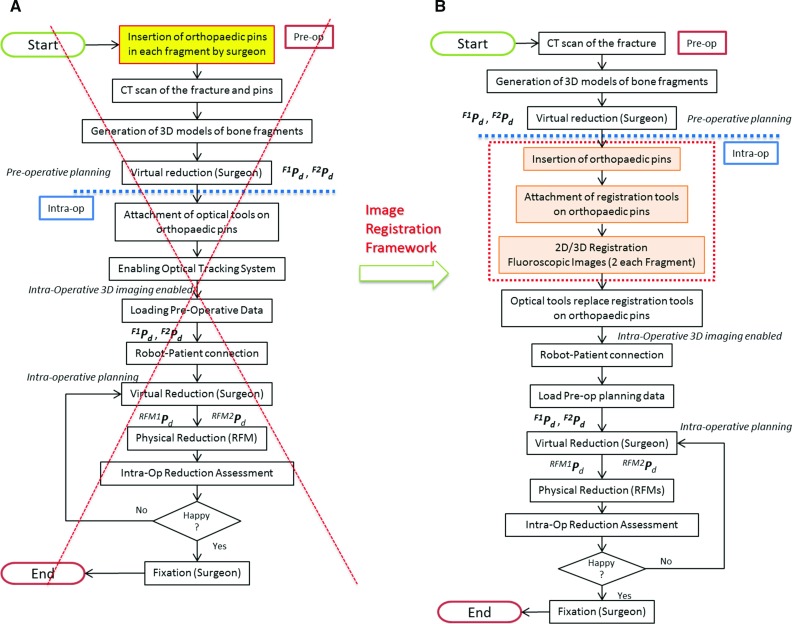
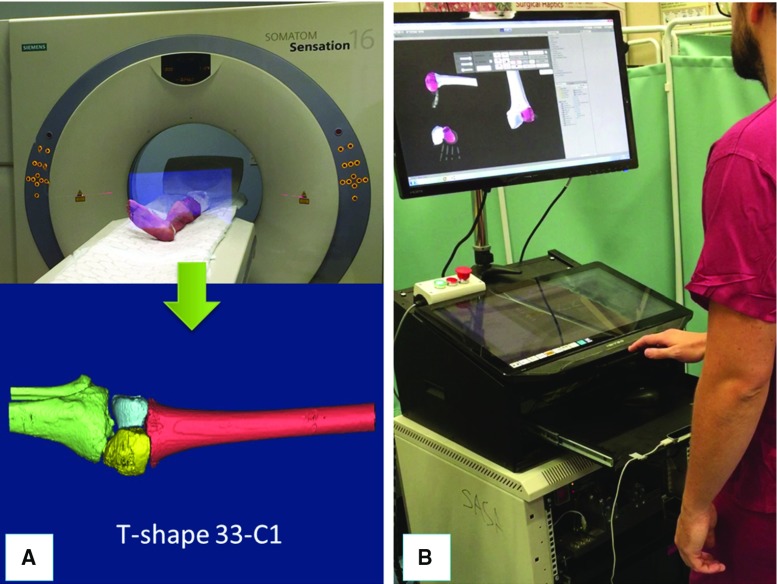
Joint fractures must be accurately reduced minimising soft tissue damages to avoid negative surgical outcomes. To this regard, we have developed the RAFS surgical system, which allows the percutaneous reduction of intra-articular fractures and provides intra-operative real-time 3D image guidance to the surgeon. Earlier experiments showed the effectiveness of the RAFS system on phantoms, but also key issues which precluded its use in a clinical application. This work proposes a redesign of the RAFS's navigation system overcoming the earlier version's issues, aiming to move the RAFS system into a surgical environment.
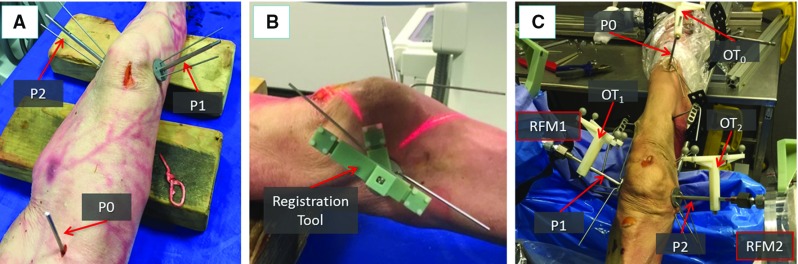
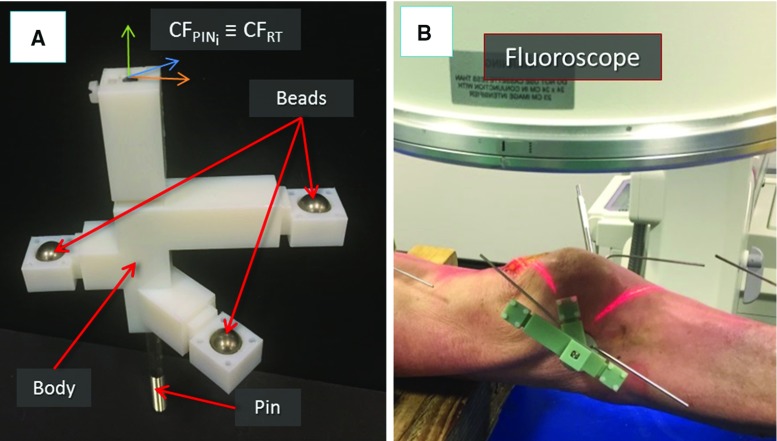
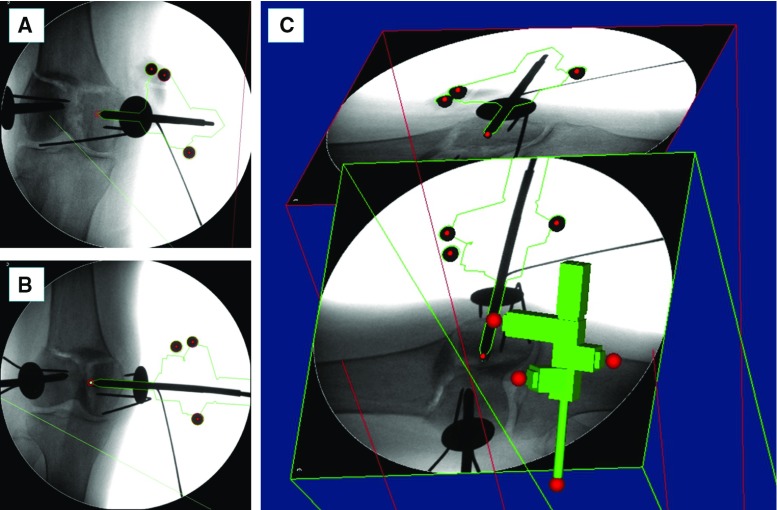
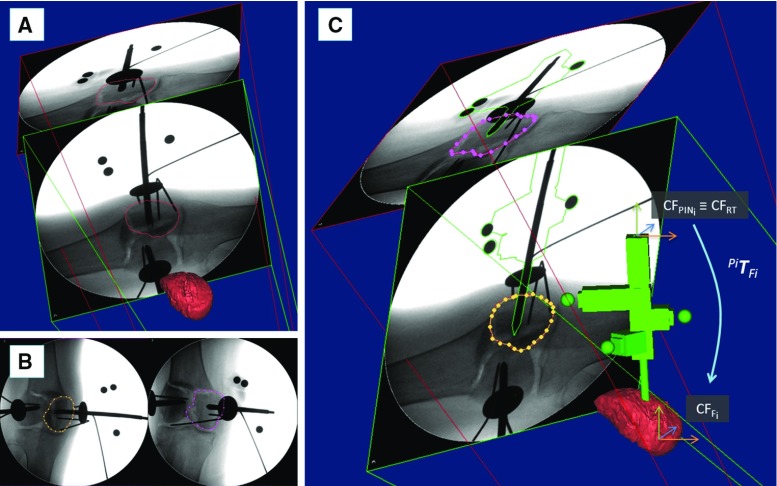
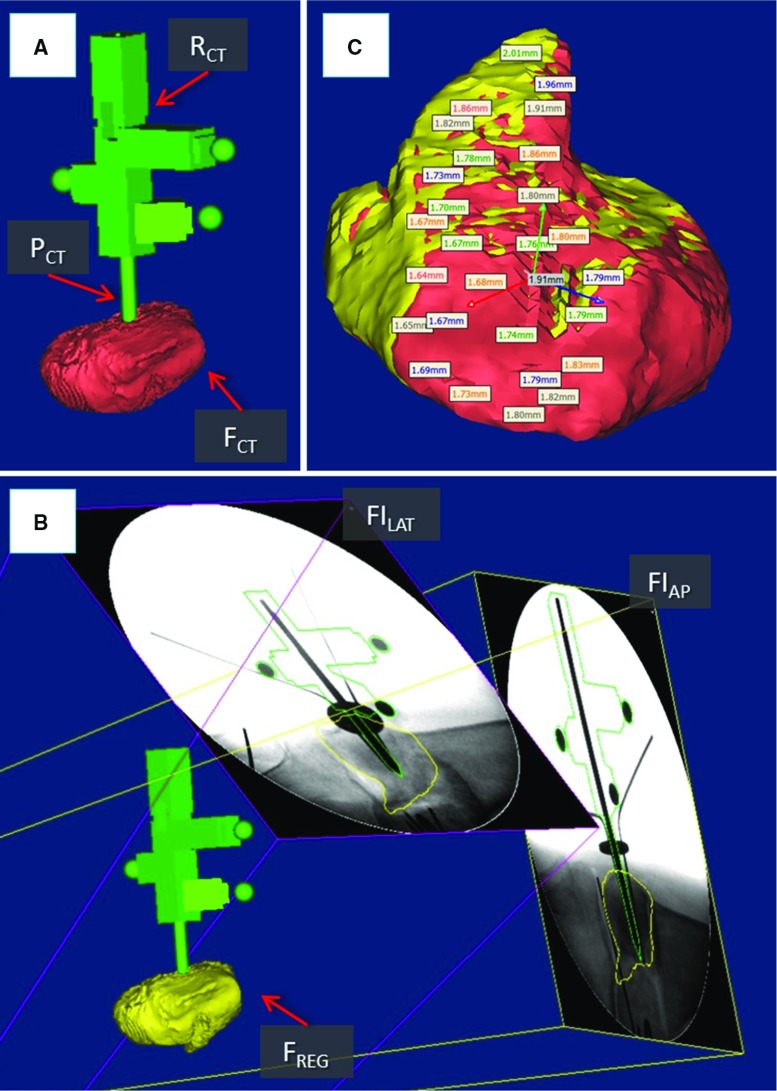
The navigation system is improved through an image registration framework allowing the intra-operative registration between pre-operative CT images and intra-operative fluoroscopic images of a fractured bone using a custom-made fiducial marker. The objective of the registration is to estimate the relative pose between a bone fragment and an orthopaedic manipulation pin inserted into it intra-operatively. The actual pose of the bone fragment can be updated in real time using an optical tracker, enabling the image guidance.
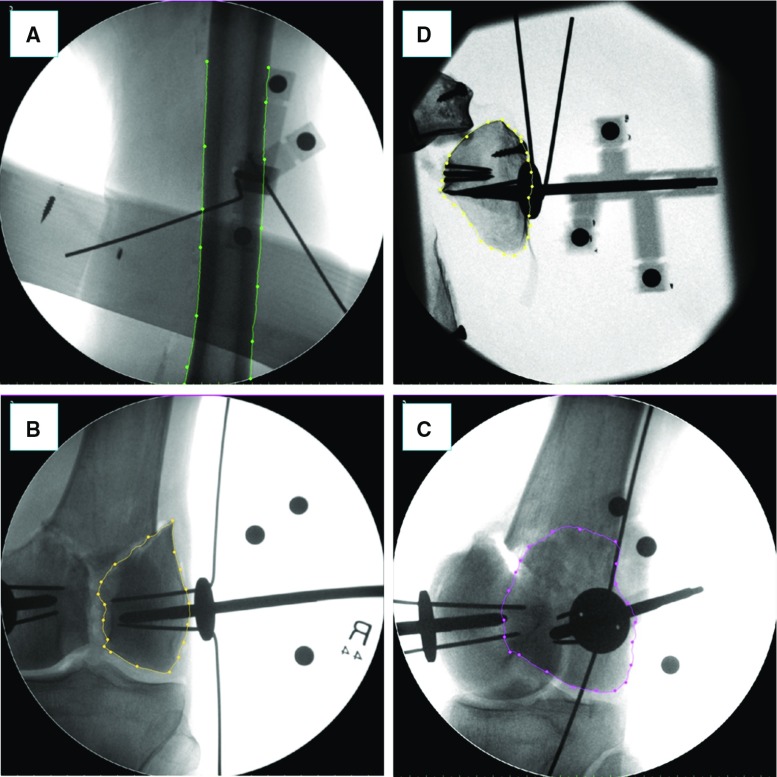
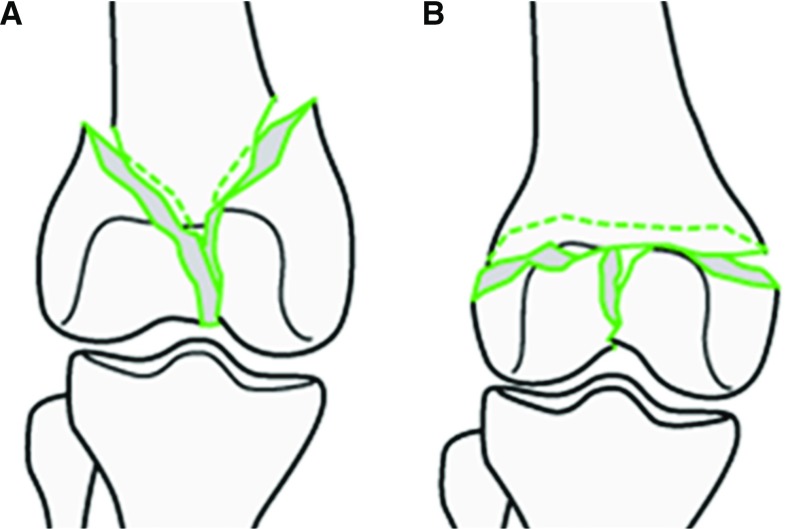
Experiments on phantom and cadavers demonstrated the accuracy and reliability of the registration framework, showing a reduction accuracy (sTRE) of about [Formula: see text] (phantom) and [Formula: see text] (cadavers). Four distal femur fractures were successfully reduced in cadaveric specimens using the improved navigation system and the RAFS system following the new clinical workflow (reduction error [Formula: see text], [Formula: see text].
Experiments showed the feasibility of the image registration framework. It was successfully integrated into the navigation system, allowing the use of the RAFS system in a realistic surgical application.
关节骨折必须精确复位,同时尽量减少软组织损伤,以避免手术出现不良后果。在这方面,我们开发了RAFS手术系统,该系统可实现关节内骨折的经皮复位,并为外科医生提供术中实时3D图像引导。早期实验表明RAFS系统在模型上有效,但也存在一些关键问题,妨碍了其在临床应用中的使用。这项工作提出对RAFS导航系统进行重新设计,以克服早期版本的问题,旨在将RAFS系统应用于手术环境。
通过一个图像配准框架改进导航系统,该框架使用定制的基准标记,实现术前CT图像与骨折骨术中透视图像之间的术中配准。配准的目的是估计骨碎片与术中插入其中的骨科操作针之间的相对位姿。骨碎片的实际位姿可使用光学跟踪器实时更新,从而实现图像引导。
在模型和尸体上进行的实验证明了配准框架的准确性和可靠性,显示复位精度(sTRE)约为[公式:见原文](模型)和[公式:见原文](尸体)。使用改进后的导航系统和RAFS系统,按照新的临床工作流程,在尸体标本中成功复位了四处股骨远端骨折(复位误差[公式:见原文],[公式:见原文])。
实验表明图像配准框架是可行的。它已成功集成到导航系统中,使得RAFS系统能够在实际手术应用中使用。