Glance Laurent G, Li Yue, Dick Andrew W
Department of Anesthesiology, University of Rochester School of Medicine, Rochester, USA.
RAND Health, RAND, Boston, USA.
BMC Health Serv Res. 2017 May 5;17(1):327. doi: 10.1186/s12913-017-2266-4.
Readmission penalties are central to the Centers for Medicare and Medicaid Services (CMS) efforts to improve patient outcomes and reduce health care spending. However, many clinicians believe that readmission metrics may unfairly penalize low-mortality hospitals because mortality and readmission are competing risks. The objective of this study is to compare hospital ranking based on a composite outcome of death or readmission versus readmission alone.
We performed a retrospective observational study of 344,565 admissions for acute myocardial infarction (AMI), congestive heart failure (CHF), or pneumoniae (PNEU) using population-based data from the New York State Inpatient Database (NY SID) between 2011 and 2013. Hierarchical logistic regression modeling was used to estimate separate risk-adjustment models for the (1) composite outcome (in-hospital death or readmission within 7-days), and (2) 7-day readmission. Hospital rankings based on the composite measure and the readmission measure were compared using the intraclass correlation coefficient and kappa analysis.
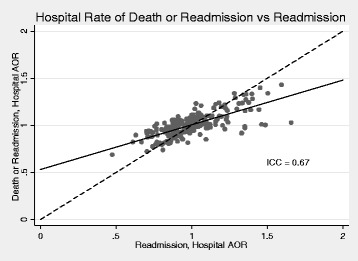
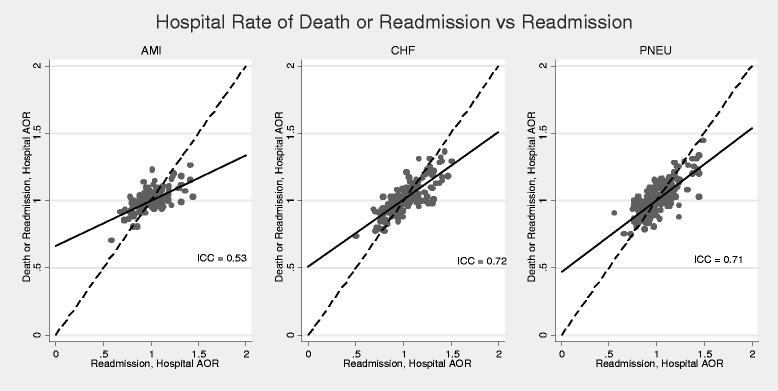
Using data from all AMI, CHF, and PNEU admissions, there was substantial agreement between hospital adjusted odds ratio (AOR) based on the composite outcome versus the readmission outcome (intraclass correlation coefficient [ICC] 0.67; 95% CI: 0.56, 0.75). For patients admitted with AMI, there was moderate agreement (ICC 0.53; 95% CI: 0.41, 0.62); for CHF, substantial agreement (ICC 0.72; 95% CI: 0.66, 0.78); and for PNEU, substantial agreement (ICC 0.71; 95% CI: 0.61, 0.78). There was moderate agreement when the composite and readmission metrics were used to classify hospitals as high, average, and low-performance hospitals (κ = 0.54, SE = 0.050). For patients admitted with AMI, there was slight agreement (κ = 0.14, SE = 0.037) between the two metrics.
Hospital performance on readmissions is significantly different from hospital performance on a composite metric based on readmissions and mortality. CMS and policy makers should consider re-assessing the use of readmission metrics for measuring hospital performance.
再入院处罚是医疗保险和医疗补助服务中心(CMS)改善患者治疗效果和降低医疗保健支出努力的核心。然而,许多临床医生认为,再入院指标可能会不公平地惩罚低死亡率医院,因为死亡率和再入院是相互竞争的风险。本研究的目的是比较基于死亡或再入院的综合结果与仅基于再入院的医院排名。
我们使用2011年至2013年纽约州住院患者数据库(NY SID)中的基于人群的数据,对344,565例急性心肌梗死(AMI)、充血性心力衰竭(CHF)或肺炎(PNEU)患者的入院情况进行了回顾性观察研究。使用分层逻辑回归模型来估计(1)综合结果(住院死亡或7天内再入院)和(2)7天再入院的单独风险调整模型。使用组内相关系数和kappa分析比较基于综合指标和再入院指标的医院排名。
使用所有AMI、CHF和PNEU入院患者的数据,基于综合结果的医院调整优势比(AOR)与再入院结果之间存在实质性一致性(组内相关系数[ICC] 0.67;95% CI:0.56,0.75)。对于AMI入院患者,存在中度一致性(ICC 0.53;95% CI:0.41,0.62);对于CHF,存在实质性一致性(ICC 0.72;95% CI:0.66,0.78);对于PNEU,存在实质性一致性(ICC 0.71;95% CI:0.61,0.78)。当使用综合指标和再入院指标将医院分类为高绩效、平均绩效和低绩效医院时,存在中度一致性(κ = 0.54,SE = 0.050)。对于AMI入院患者,两种指标之间存在轻微一致性(κ = 0.14,SE = 0.037)。
医院在再入院方面的表现与基于再入院和死亡率的综合指标的医院表现存在显著差异。CMS和政策制定者应考虑重新评估使用再入院指标来衡量医院绩效。