Hunasgi Santosh, Koneru Anila, Vanishree M, Manvikar Vardendra
Department of Oral and Maxillofacial Pathology, Navodaya Dental College, Raichur, Karnataka, India.
J Oral Maxillofac Pathol. 2017 Jan-Apr;21(1):180. doi: 10.4103/jomfp.JOMFP_23_16.
In the literature, many studies were attempted to analyze the distribution of oral reactive lesions in terms of age, gender and location. However, very few studies have focused on the detailed histopathological features of these reactive lesions of oral cavity. Thus, the purpose of this paper is to document the occurrence, distribution and various histopathological features of reactive gingival lesions.
This study is a retrospective archival review of reactive gingival lesions of oral cavity such as irritational fibroma (IF), inflammatory gingival hyperplasia (IGF), pyogenic granuloma (PG), peripheral giant cell granuloma (PGCG) and peripheral ossifying fibroma involving gingival tissues. All the cases were histopathologically reviewed on some microscopical parameters according to the criteria given by Peralles .
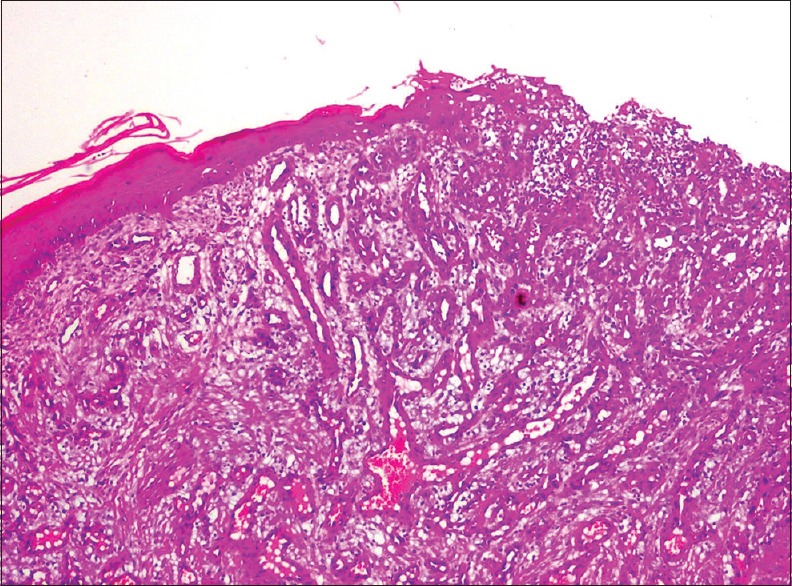
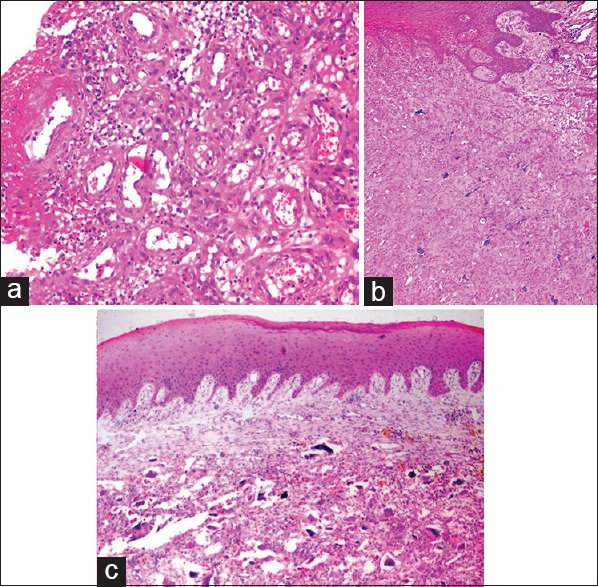
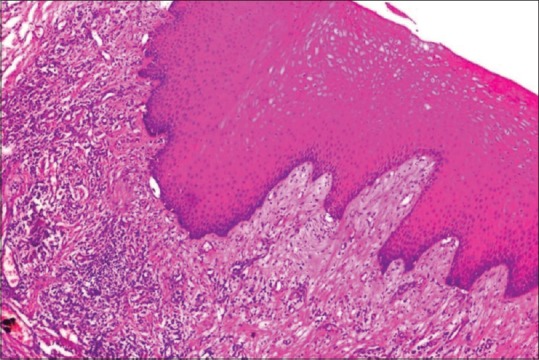
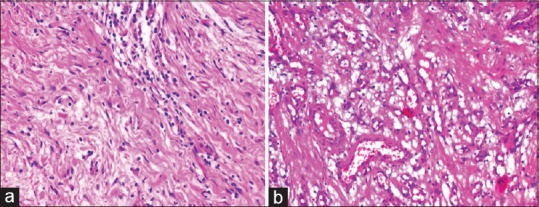
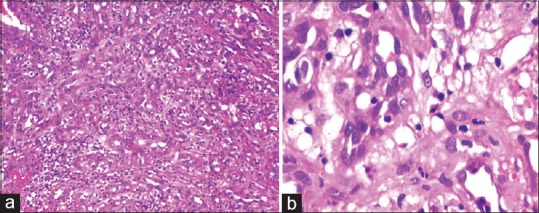
Regarding epithelial morphology, atrophy, ulceration and hyperplasia were found predominantly in PG. Connective tissue was predominantly dense in IGF and IF with fibroblastic proliferation; whereas loose connective tissue was seen in PG. Vascular proliferation, especially capillary, was commonly present in PG and inflammatory gingival hyperplasia (IGH). Inflammatory cell infiltrate was intense in both PG and IGH. Mineralization showed a marked affinity for peripheral cement-ossifying fibroma, and bone/bone-like areas were found in about ten cases of them. The Foreign body type of multinucleated giant cells was found exclusively on PGCG.
Despite their clinical similarities, the findings of this study reports that all reactive gingival lesions show some differences in age, type, location, duration and histopathological features. Nevertheless, the differing histological pictures are a range of a single lesion in diverse stages of maturation. Essential in the treatment of reactive lesions is the total removal of the lesion with local irritants such as defective restorations or calculus formation.
在文献中,许多研究试图从年龄、性别和部位方面分析口腔反应性病变的分布情况。然而,很少有研究关注这些口腔反应性病变的详细组织病理学特征。因此,本文的目的是记录反应性牙龈病变的发生情况、分布及各种组织病理学特征。
本研究是对口腔反应性牙龈病变进行回顾性存档分析,这些病变包括刺激性纤维瘤(IF)、炎症性牙龈增生(IGF)、化脓性肉芽肿(PG)、外周巨细胞肉芽肿(PGCG)以及累及牙龈组织的外周骨化性纤维瘤。所有病例均根据佩拉莱斯给出的标准,在一些微观参数方面进行组织病理学复查。
关于上皮形态,萎缩、溃疡和增生主要见于化脓性肉芽肿。炎症性牙龈增生和刺激性纤维瘤的结缔组织主要致密,伴有成纤维细胞增生;而化脓性肉芽肿中可见疏松结缔组织。血管增生,尤其是毛细血管增生,常见于化脓性肉芽肿和炎症性牙龈增生。化脓性肉芽肿和炎症性牙龈增生中炎症细胞浸润均很明显。矿化在外周牙骨质 - 骨化性纤维瘤中表现出显著相关性,约10例病例中发现有骨/类骨区域。异物型多核巨细胞仅在外周巨细胞肉芽肿中发现。
尽管这些病变在临床上有相似之处,但本研究结果表明,所有反应性牙龈病变在年龄、类型、部位、病程和组织病理学特征方面均存在一些差异。然而,不同的组织学表现是同一病变在不同成熟阶段的一系列表现。治疗反应性病变的关键在于彻底切除病变及去除局部刺激因素,如修复体不良或牙结石形成。