Whittaker Elizabeth, Nicol Mark, Zar Heather J, Kampmann Beate
Academic Department of Paediatrics, Imperial College London, London, UK.
UCT Faculty of Health Sciences, Division of Medical Microbiology, Department of Clinical Laboratory Sciences, Institute of Infectious Disease and Molecular Medicine, Cape Town, South Africa.
Front Immunol. 2017 Apr 25;8:448. doi: 10.3389/fimmu.2017.00448. eCollection 2017.
Following infection with (M.tb), children are more susceptible to develop disease particularly extrapulmonary disease than adults. The exact mechanisms required for containment of M.tb are not known, but would be important to identify correlates of protection.
To comprehensively analyze key immune responses to mycobacteria between HIV-negative children with extrapulmonary TB (EPTB) compared to children with pulmonary TB (PTB) or healthy controls.
Whole blood was stimulated with mycobacteria for 24 h or 6 days to induce effector and memory responses. CD4, CD8, γδ, regulatory T cells, and their related cytokines were measured. Samples of children with tuberculosis (TB) disease were analyzed both at time of diagnosis and at the end of TB treatment to determine if any differences were due to TB disease or an underlying host phenotype.
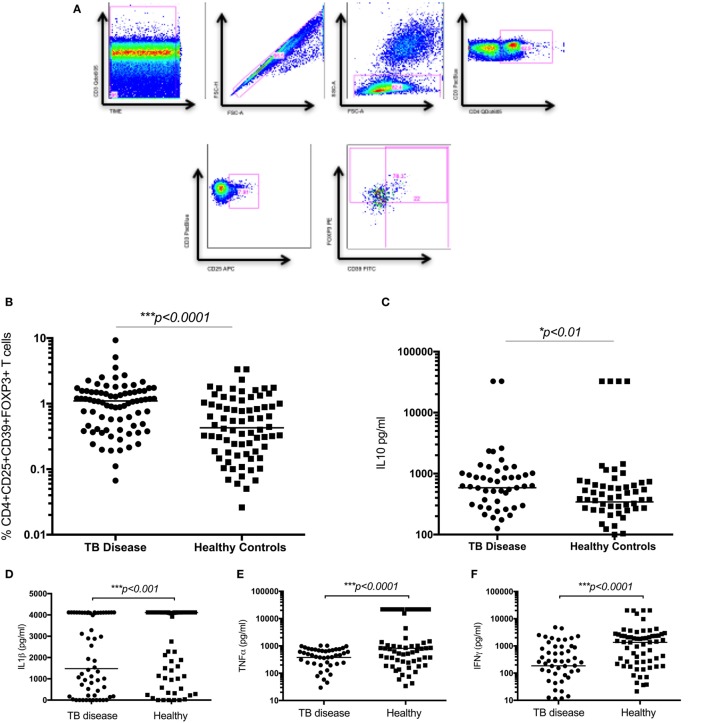
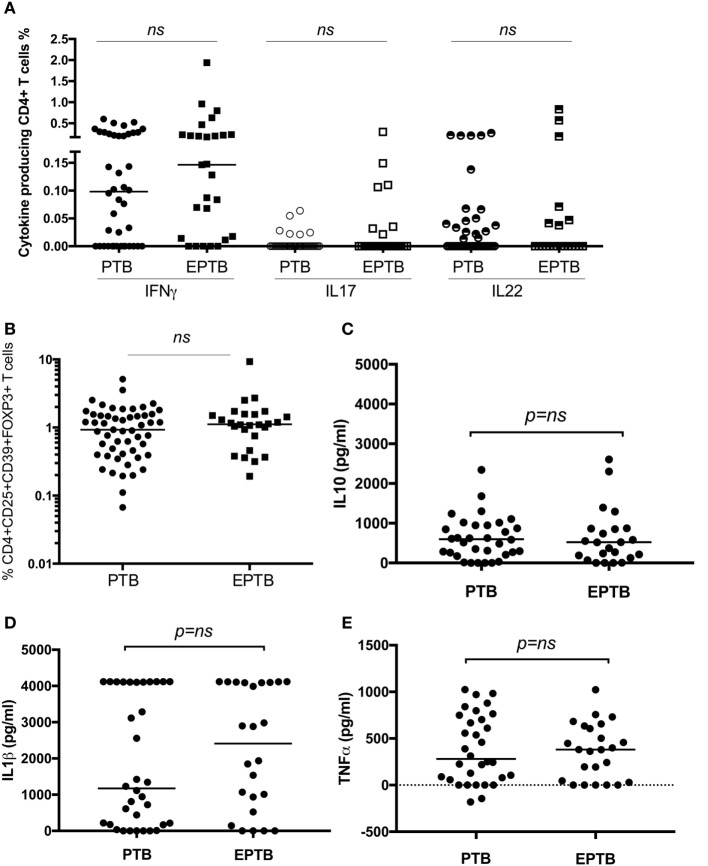
Seventy-six children with TB disease (48 with PTB and 28 with EPTB) and 83 healthy controls were recruited to the study. The frequency of CD4CD25CD39FOXP3 regulatory T cells and secreted IL10 were significantly higher in children with TB compared to healthy controls. IFNγ-, IL17-, and IL22-producing γδ T cells, IL22-producing CD4 T cells and secreted pro-inflammatory cytokines (IFNγ, IL1β, and TNFα) were significantly lower in children with TB disease compared to healthy controls. IFNγ-producing CD4 T cells and Ki67-proliferating CD4 T cells, however, were present in equal numbers in both groups. Following treatment, these immune parameters recovered to "healthy" levels or greater in children with PTB, but not those with extrapulmonary TB.
In children with TB disease, a predominantly immune regulatory state is present. These immune findings do not distinguish between children with PTB and EPTB at the time of diagnosis. Following treatment, these inflammatory responses recover in PTB, suggesting that the effect is disease specific rather than due to an underlying host defect.
感染结核分枝杆菌(M.tb)后,儿童比成人更容易患疾病,尤其是肺外疾病。控制结核分枝杆菌所需的确切机制尚不清楚,但确定保护的相关因素很重要。
全面分析与肺结核(PTB)儿童或健康对照相比,肺外结核(EPTB)的HIV阴性儿童对分枝杆菌的关键免疫反应。
用分枝杆菌刺激全血24小时或6天以诱导效应和记忆反应。测量CD4、CD8、γδ、调节性T细胞及其相关细胞因子。对结核病患儿的样本在诊断时和结核病治疗结束时进行分析,以确定是否有任何差异是由于结核病本身还是潜在的宿主表型。
76例结核病患儿(48例PTB和28例EPTB)和83名健康对照被纳入研究。与健康对照相比,结核病患儿中CD4CD25CD39FOXP3调节性T细胞的频率和分泌的IL10显著更高。与健康对照相比,结核病患儿中产生IFNγ、IL17和IL22的γδT细胞、产生IL22的CD4T细胞以及分泌的促炎细胞因子(IFNγ、IL1β和TNFα)显著更低。然而,两组中产生IFNγ的CD4T细胞和Ki67增殖的CD4T细胞数量相等。治疗后,PTB患儿的这些免疫参数恢复到“健康”水平或更高,但肺外结核患儿则不然。
在结核病患儿中,存在主要为免疫调节的状态。这些免疫结果在诊断时无法区分PTB和EPTB患儿。治疗后,PTB患儿的这些炎症反应恢复,表明这种效应是疾病特异性的,而非由于潜在的宿主缺陷。