Claus Christiano Marlo Paggi, Nassif Lucas Thá, Aguilera Yan Sacha, Ramos EduardoJose Brommelstroet, Coelho Julio Cesar Uili
Nossa Senhora das Graças Hospital.
Service of Digestive System Surgery and Jacques Perissat Institute, Universidade Positivo, Curitiba, PR, Brazil.
Arq Bras Cir Dig. 2017 Jan-Mar;30(1):56-59. doi: 10.1590/0102-6720201700010016.
: Lumbar hernias are rare. Usually manifest with reducible volume increase in the post-lateral region of the abdomen and may occur in two specific anatomic defects: the triangles of Grynfelt (upper) and Petit (lower). Despite controversies with better repair, laparoscopic approach, following the same principle of the treatment of inguinal hernias, seems to present significant advantages compared to conventional/open surgeries. However, some technical and anatomical details of the region, non usual to general surgeons, are fundamental for proper repair.
: To present systematization of laparoscopic transabdominal technique for repair of lumbar hernias with emphasis on anatomical details.
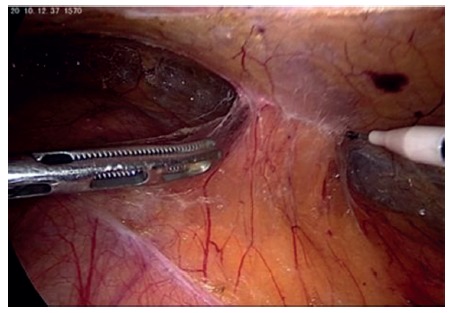
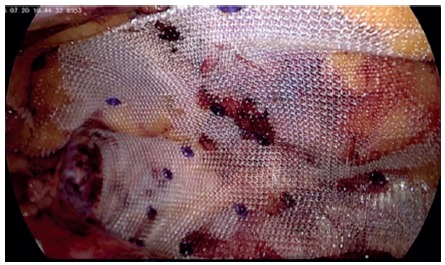
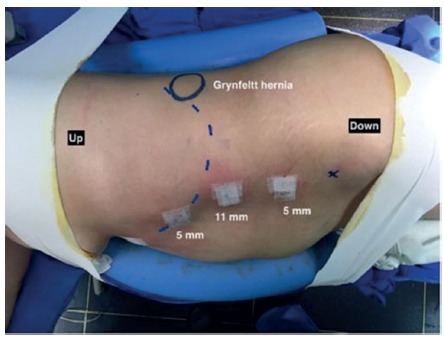
: Patient is placed in the lateral decubitus. Laparoscopic access to abdominal cavity is performed by open technique on the left flank, 1.5 cm incision, followed by introduction of 11 mm trocar for a 30º scope. Two other 5 mm trocars, in the left anterior axillary line, are inserted into the abdominal cavity. The peritoneum of the left paracolic gutter is incised from the 10th rib to the iliac crest. Peritoneum and retroperitoneal is dissected. Reduction of all hernia contents is performed to demonstrate the hernia and its size. A 10x10 cm polypropylene mesh is introduced into the retroperitoneal space and fixed with absorbable staples covering the defect with at least 3-4 cm overlap. Subsequently, is carried out the closure of the peritoneum of paracolic gutter.
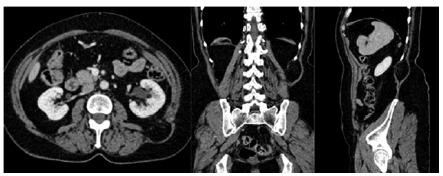
: This technique was used in one patient with painful increased volume in the left lower back and bulging on the left lumbar region. CT scan was performed and revealed left superior lumbar hernia. Operative time was 45 min and there were no complications and hospitalization time of 24 h.
: As in inguinal hernia repair, laparoscopic approach is safe and effective for the repair of lumbar hernias, especially if the anatomical details are adequately respected.
: As hérnias lombares são raras. Geralmente se manifestam com aumento de volume redutível na região póstero-lateral do abdome e podem ocorrer em dois defeitos anatômicos específicos: os triângulos de Grynfelt (superior) e Petit (inferior). Apesar de controvérsias com relação a melhor forma de reparo, a abordagem laparoscópica, seguindo o mesmo princípio do tratamento das hérnias inguinais, parece apresentar vantagens significativas em relação às operações convencionais/abertas. Entretanto, alguns detalhes técnicos e anatômicos desta região, não usual aos cirurgiões gerais, são fundamentais para o adequado reparo.
: Apresentar sistematização da técnica laparoscópica transabdominal para a correção das hérnias lombares com ênfase nos detalhes anatômicos.
MÉTODO:: Paciente é colocado em decúbito lateral. O acesso laparoscópico à cavidade abdominal é realizado pela técnica aberta no flanco esquerdo, incisão de 1,5 cm, seguida pela introdução de trocárteres de 11 mm para ótica de 30º. Dois outros trocárteres de 5 mm, na linha axilar anterior esquerda, são inseridos na cavidade abdominal. O peritônio da goteira paracólica esquerda é incisado desde a 10ª costela até a crista ilíaca. O peritônio e o retroperitoneal são dissecados. A redução de todo o conteúdo de hérnia é realizada para demonstrar a hérnia e seu tamanho. Tela de polipropileno de 10x10 cm é introduzida no espaço retroperitoneal e fixada com grampos absorvíveis cobrindo o defeito com pelo menos 3-4 cm de sobreposição. Posteriormente, realiza-se o fechamento do peritônio da goteira paracólica.
: Esta técnica foi utilizada em um paciente com aumento doloroso de volume na região lombar esquerda e abaulamento na região lombar esquerda. Tomografia computadorizada foi realizada e revelou hérnia lombar superior esquerda. O tempo operatório foi de 45 min e não houve complicações; o tempo de hospitalização de 24 h.
CONCLUSÕES:: Assim como no reparo das hérnias inguinais, a abordagem laparoscópica é segura e efetiva para as hérnias lombares, especialmente se os detalhes anatômicos forem adequadamente respeitados.
腰椎疝较为罕见。通常表现为腹部后侧区域可复性体积增大,可发生于两个特定的解剖缺损部位:格伦费尔特三角(上部)和佩蒂三角(下部)。尽管在最佳修复方式上存在争议,但腹腔镜手术遵循与腹股沟疝治疗相同的原则,与传统/开放手术相比似乎具有显著优势。然而,该区域一些普通外科医生不常见的技术和解剖细节对于正确修复至关重要。
介绍腹腔镜经腹技术修复腰椎疝的系统化方法,重点关注解剖细节。
患者取侧卧位。通过左侧腰部开放式技术进入腹腔,切口1.5厘米,随后插入11毫米套管针用于30°腹腔镜。在左腋前线再插入另外两个5毫米套管针进入腹腔。切开左结肠旁沟的腹膜,从第10肋至髂嵴。分离腹膜和腹膜后组织。将所有疝内容物回纳以显示疝及其大小。将一块10×10厘米的聚丙烯补片放入腹膜后间隙,用可吸收吻合钉固定,覆盖缺损部位并至少重叠3 - 4厘米。随后,缝合结肠旁沟的腹膜。
该技术应用于一名左下背部疼痛性体积增大且左腰部膨隆的患者。进行了CT扫描,显示为左上腰椎疝。手术时间为45分钟,无并发症,住院时间为24小时。
与腹股沟疝修复一样,腹腔镜手术修复腰椎疝安全有效,尤其是在充分尊重解剖细节的情况下。
腰椎疝较为罕见。通常表现为腹部后侧区域可复性体积增大,可发生于两个特定的解剖缺损部位:格伦费尔特三角(上部)和佩蒂三角(下部)。尽管在最佳修复方式上存在争议,但腹腔镜手术遵循与腹股沟疝治疗相同的原则,与传统/开放手术相比似乎具有显著优势。然而,该区域一些普通外科医生不常见的技术和解剖细节对于正确修复至关重要。
介绍腹腔镜经腹技术修复腰椎疝的系统化方法,重点关注解剖细节。
患者取侧卧位。通过左侧腰部开放式技术进入腹腔,切口1.5厘米,随后插入11毫米套管针用于30°腹腔镜。在左腋前线再插入另外两个5毫米套管针进入腹腔。切开左结肠旁沟的腹膜,从第10肋至髂嵴。分离腹膜和腹膜后组织。将所有疝内容物回纳以显示疝及其大小。将一块10×10厘米的聚丙烯补片放入腹膜后间隙,用可吸收吻合钉固定,覆盖缺损部位并至少重叠3 - 4厘米。随后,缝合结肠旁沟的腹膜。
该技术应用于一名左下背部疼痛性体积增大且左腰部膨隆的患者。进行了CT扫描,显示为左上腰椎疝。手术时间为45分钟,无并发症,住院时间为24小时。
与腹股沟疝修复一样,腹腔镜手术修复腰椎疝安全有效,尤其是在充分尊重解剖细节的情况下。